

Trends in US Emergency Department Visits for Pediatric Acute Ocular Injury
- PMID: 29879287
- PMCID: PMC6142941
- DOI: 10.1001/jamaophthalmol.2018.2062
Trends in US Emergency Department Visits for Pediatric Acute Ocular Injury
Erratum in
-
Error in Key Points.JAMA Ophthalmol. 2018 Aug 1;136(8):959. doi: 10.1001/jamaophthalmol.2018.2944. JAMA Ophthalmol. 2018. PMID: 30003223 Free PMC article. No abstract available.
Abstract
Importance: There is a lack of literature describing the incidence of pediatric acute ocular injury and associated likelihood of vision loss in the United States. Understanding national pediatric eye injury trends may inform future efforts to prevent ocular trauma.
Objective: To characterize pediatric acute ocular injury in the United States using data from a stratified, national sample of emergency department (ED) visits.
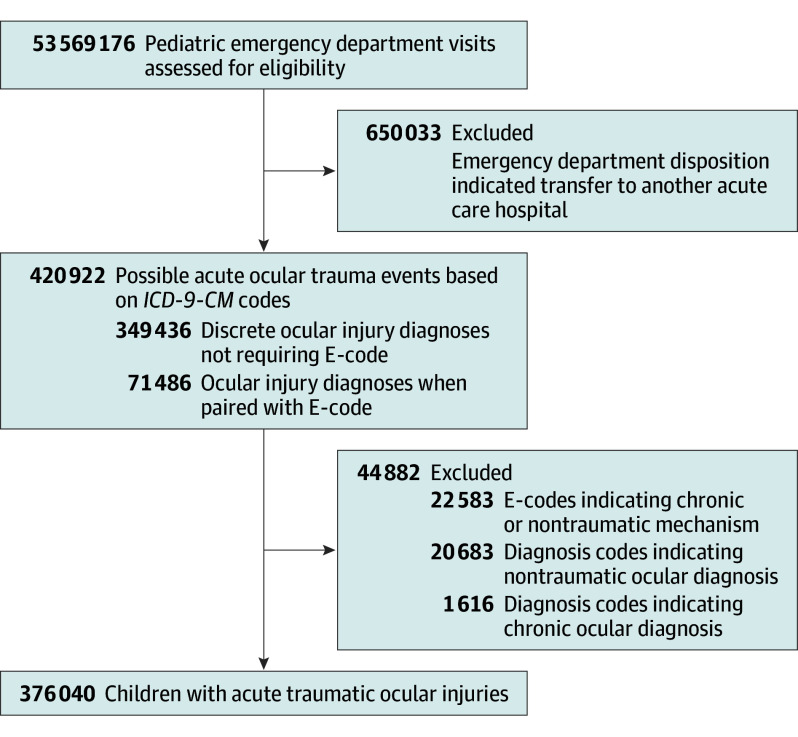
Design, setting, and participants: A retrospective cohort study was conducted. Study participants received care at EDs included in the 2006 to 2014 Nationwide Emergency Department Sample, comprising 376 040 children aged 0 to 17 years with acute traumatic ocular injuries. Data were analyzed from June 2016 to March 2018.
Exposures: International Classification of Diseases, Ninth Revision, Clinical Modification diagnosis codes and external-cause-of-injury codes identified children with acute ocular injuries.
Main outcomes and measures: Demographic and clinical characteristics of children with acute traumatic ocular injuries were collected and temporal trends in the incidence of ocular injuries by age, risk of vision loss, and mechanism of injury were explored.
Results: In 2014, there were an estimated 163 431 (95% CI, 151 235-175 627) ED visits for pediatric acute ocular injury. Injured children were more often male (63.0%; 95% CI, 62.5-63.5) and in the youngest age category (birth to 4 years, 35.3%; 95% CI, 34.4-36.2; vs 10-14 years, 20.6%; 95% CI, 20.1-21.1). Injuries commonly resulted from a strike to the eye (22.5%; 95% CI, 21.3-23.8) and affected the adnexa (43.7%; 95% CI, 42.7-44.8). Most injuries had a low risk for vision loss (84.2%; 95% CI, 83.5-85.0), with only 1.3% (95% CI, 1.1-1.5) of injuries being high risk. Between 2006 and 2014, pediatric acute ocular injuries decreased by 26.1% (95% CI, -27.0 to -25.0). This decline existed across all patient demographic characteristics, injury patterns, and vision loss categories and for most mechanisms of injury. There were increases during the study in injuries related to sports (12.8%; 95% CI, 5.4-20.2) and household/domestic activities (20.7%; 95% CI, 16.2-25.2). The greatest decrease in high-risk injuries occurred with motor vehicle crashes (-79.8%; 95% CI, -85.8 to -74.9) and guns (-68.5%; 95% CI, -73.5 to -63.6).
Conclusions and relevance: This study demonstrated a decline in pediatric acute ocular injuries in the United States between 2006 and 2014. However, pediatric acute ocular injuries continue to be prevalent, and understanding these trends can help establish future prevention strategies.
Conflict of interest statement
Figures
Comment in
-
Uncovering Reasons Why Acute Ocular Injuries in Children May Be Declining.JAMA Ophthalmol. 2018 Aug 1;136(8):904. doi: 10.1001/jamaophthalmol.2018.2059. JAMA Ophthalmol. 2018. PMID: 29879282 No abstract available.
References
-
- Owens PL, Mutter R. Emergency department visits related to eye injuries, 2008: statistical brief #112. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb112.pdf. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Accessed November 3, 2017.
-
- Rui P, Kang K. National Hospital Ambulatory Medical Care Survey: 2014 emergency department summary tables. https://www.cdc.gov/nchs/data/nhamcs/web_tables/2014_ed_web_tables.pdf. Accessed May 1, 2018.
-
- Negral AD. Magnitude of eye injuries worldwide. Comm Eye Health. 1997;10(24):49-53.
-
- Acuna OM, Yen KG. Outcome and prognosis of pediatric patients with delayed diagnosis of open-globe injuries. J Pediatr Ophthalmol Strabismus. 2009;46(4):202-207. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
