

Influence of Skeletal Muscle Mass and Spinal Alignment on Surgical Outcomes for Lumbar Spinal Stenosis
- PMID: 29879785
- PMCID: PMC6002163
- DOI: 10.4184/asj.2018.12.3.556
Influence of Skeletal Muscle Mass and Spinal Alignment on Surgical Outcomes for Lumbar Spinal Stenosis
Abstract
Study design: Retrospective observational study.
Purpose: We considered the relationship between spinal alignment and skeletal muscle mass on clinical outcomes following a surgery for lumbar spinal stenosis (LSS).
Overview of literature: There are no reports of preoperative factors predicting residual low back pain following surgery for LSS.
Methods: Our target population included 34 women (mean age, 74.4 years) who underwent surgery for LSS. Prior to and 6 months after the surgery, systemic bone mineral density and lean soft tissue mass were measured using dual-energy X-ray absorptiometry. Skeletal muscle mass index (SMI) was calculated as the sum of the arm and leg lean mass in kilograms divided by height in meters squared. The spinal alignment was also measured. Clinical outcomes were evaluated using the Japanese Orthopedic Association scoring system, leg and low back pain Visual Analog Scale, and Roland-Morris Disability Questionnaire (RDQ). Additionally, we examined the bone mineral density, skeletal muscle mass, and spinal alignment before and after the surgery. We used the Spearman correlation coefficient to examine the associations among clinical outcomes, preoperative muscle mass, and spinal alignment.
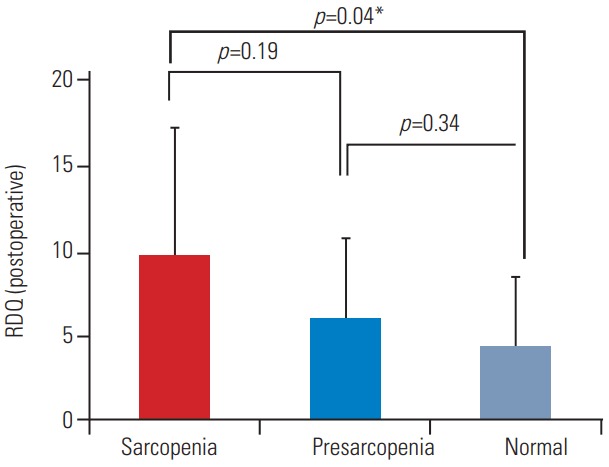
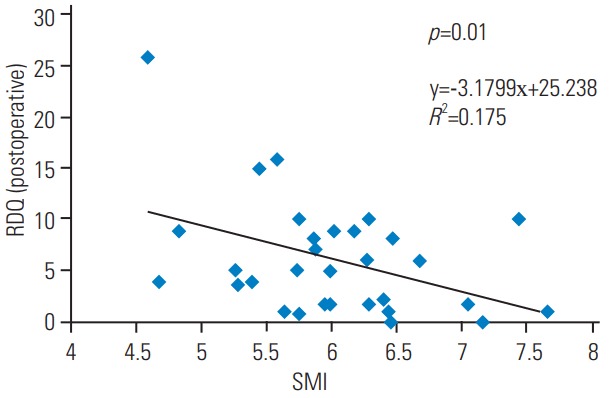
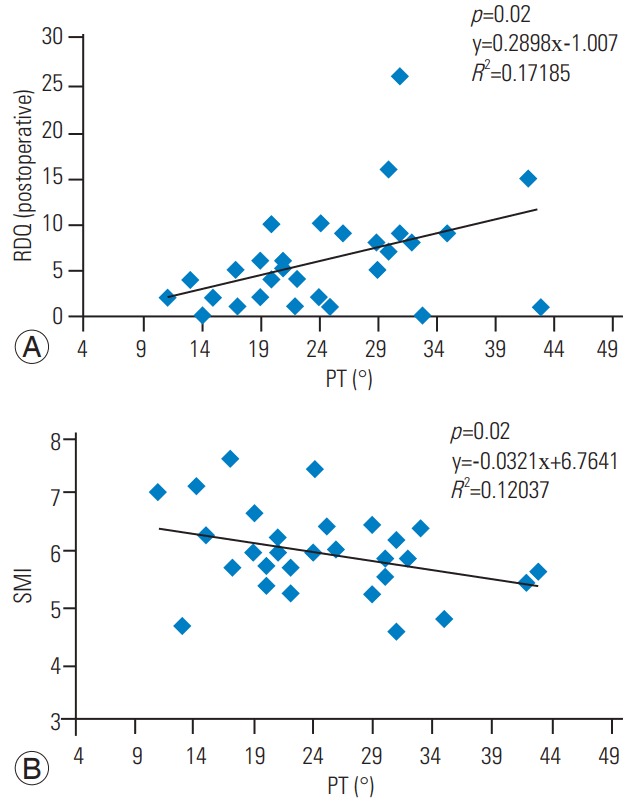
Results: Sarcopenia (SMI <5.46) was observed in nine subjects (26.5%). Compared with normal subjects (SMI >6.12), RDQ was significantly higher in subjects with sarcopenia (p =0.04). RDQ was significantly negatively correlated with SMI (r =-0.42, p <0.05). There was a significant positive correlation between postoperative RDQ and pelvic tilt (PT; r =0.41, p <0.05). SMI and PT were significantly negatively correlated (r =-0.39, r <0.05).
Conclusions: Good postoperative outcomes were negatively correlated with low preoperative appendicular muscle mass, suggesting that postoperative outcomes were inferior in cases of decreased appendicular muscle mass (sarcopenia). Posterior PT due to decreased limb muscle mass may contribute to postoperative back pain, showing that preoperatively reduced limb muscle mass and posterior PT are predictive factors in the persistence of postoperative low back pain.
Keywords: Low back pain; Sarcopenia; Skeletal muscle; Spinal stenosis; Surgery.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Associations between sarcopenia and degenerative lumbar scoliosis in older women.Scoliosis Spinal Disord. 2017 Mar 16;12:9. doi: 10.1186/s13013-017-0116-0. eCollection 2017. Scoliosis Spinal Disord. 2017. PMID: 28331906 Free PMC article.
-
Potential Role of Paraspinal Musculature in the Maintenance of Spinopelvic Alignment in Patients With Adult Spinal Deformities.Clin Spine Surg. 2020 Mar;33(2):E76-E80. doi: 10.1097/BSD.0000000000000862. Clin Spine Surg. 2020. PMID: 31385849
-
Impact of sagittal spinopelvic alignment on clinical outcomes after decompression surgery for lumbar spinal canal stenosis without coronal imbalance.J Neurosurg Spine. 2015 Oct;23(4):451-8. doi: 10.3171/2015.1.SPINE14642. Epub 2015 Jul 3. J Neurosurg Spine. 2015. PMID: 26140404
-
Evaluation of Spinal Alignment and Clinical Findings for the Efficacy of One-Stage Surgery in Tandem Spinal Stenosis.Cureus. 2022 May 19;14(5):e25130. doi: 10.7759/cureus.25130. eCollection 2022 May. Cureus. 2022. PMID: 35733489 Free PMC article.
-
Clinical Value of Muscle Mass Assessment in Clinical Conditions Associated with Malnutrition.J Clin Med. 2019 Jul 17;8(7):1040. doi: 10.3390/jcm8071040. J Clin Med. 2019. PMID: 31319519 Free PMC article. Review.
Cited by
-
Preoperative cross-sectional area of psoas muscle correlates with short-term functional outcomes after posterior lumbar surgery.Eur Spine J. 2023 Jul;32(7):2326-2335. doi: 10.1007/s00586-023-07533-7. Epub 2023 Apr 3. Eur Spine J. 2023. PMID: 37010611
-
Prevalence and Characteristics of Spinal Sagittal Malalignment in Patients with Osteoporosis.J Clin Med. 2021 Jun 26;10(13):2827. doi: 10.3390/jcm10132827. J Clin Med. 2021. PMID: 34206898 Free PMC article.
-
Preoperative Multifidus Muscle Quality is Associated With Patient Reported Outcomes After Lateral Lumbar Interbody Fusion.Global Spine J. 2024 Mar;14(2):647-656. doi: 10.1177/21925682221120400. Epub 2022 Aug 19. Global Spine J. 2024. PMID: 35984823 Free PMC article.
-
The Prevalence of Sarcopenia and Its Impact on Clinical Outcomes in Lumbar Degenerative Spine Disease-A Systematic Review and Meta-Analysis.J Clin Med. 2021 Feb 15;10(4):773. doi: 10.3390/jcm10040773. J Clin Med. 2021. PMID: 33671958 Free PMC article. Review.
-
Impact of Sarcopenia on Clinical Outcomes of Minimally Invasive Lumbar Decompression Surgery.Sci Rep. 2019 Nov 12;9(1):16619. doi: 10.1038/s41598-019-53053-0. Sci Rep. 2019. PMID: 31719579 Free PMC article.
References
-
- Ganz JC. Lumbar spinal stenosis: postoperative results in terms of preoperative posture-related pain. J Neurosurg. 1990;72:71–4. - PubMed
-
- La Grone MO. Loss of lumbar lordosis: a complication of spinal fusion for scoliosis. Orthop Clin North Am. 1988;19:383–93. - PubMed
-
- Kostuik JP, Maurais GR, Richardson WJ, Okajima Y. Combined single stage anterior and posterior osteotomy for correction of iatrogenic lumbar kyphosis. Spine (Phila Pa 1976) 1988;13:257–66. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
