

Mortality and associated factors of patients with extensive drug-resistant tuberculosis: an emerging public health crisis in China
- PMID: 29879908
- PMCID: PMC5992859
- DOI: 10.1186/s12879-018-3169-7
Mortality and associated factors of patients with extensive drug-resistant tuberculosis: an emerging public health crisis in China
Abstract
Background: Limited treatment options of extensive drug-resistant tuberculosis (XDR-TB) have led to its high mortality worldwide. Relevant data about mortality of XDR-TB patients in literature are limited and likely underestimate the real situation in China, since the majority of patients with XDR-TB are lost to follow-up after discharge from TB hospitals. In this study, we sought to investigate the mortality and associated risk factors of Human Immunodeficiency Virus (HIV)-negative patients with XDR-TB in China.
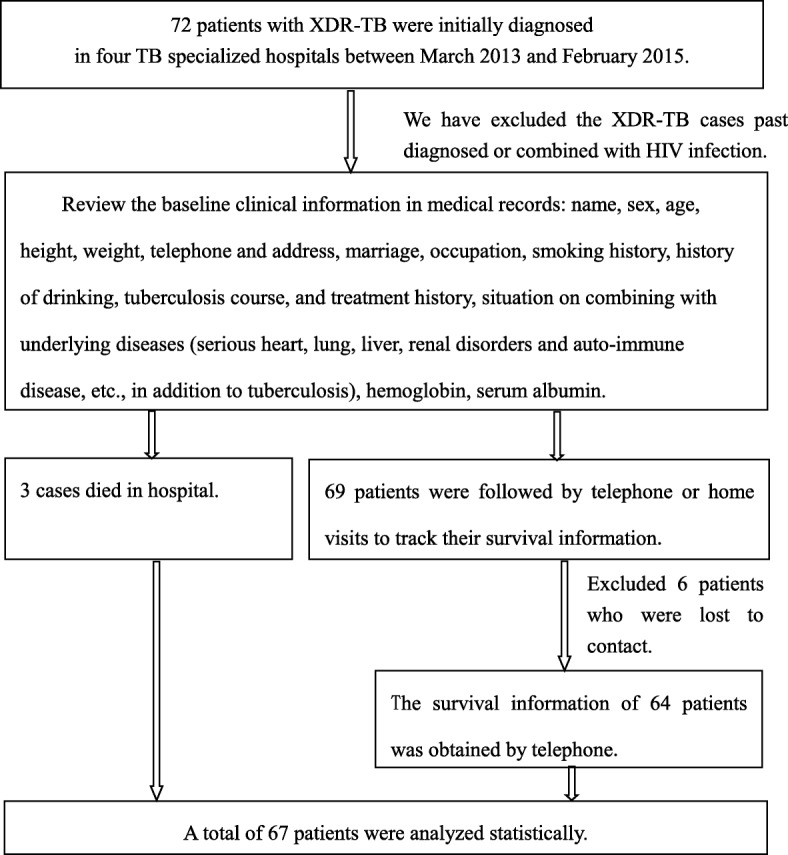
Methods: All patients who were diagnosed with XDR-TB for the first time in four TB care centers across China between March 2013 and February 2015 were consecutively enrolled. Active tracking through contacting patients or family members by phone or home visit was conducted to obtain patients' survival information by February 2017. Multivariable Cox regression models were used to evaluate factors associated with mortality.
Results: Among 67 patients enrolled, the mean age was 48.7 (Standard Deviation [SD] = 16.7) years, and 51 (76%) were men. Fourteen patients (21%) were treatment naïve at diagnosis indicating primary transmission. 58 (86.8%) patients remained positive for sputum smear or culture when discharged. During a median follow-up period of 32 months, 20 deaths occurred, with an overall mortality of 128 per 1000 person-years. Among patients who were dead, the median survival was 5.4 months (interquartile range [IQR]: 2.2-17.8). Seventeen (85%) of them died at home, among whom the median interval from discharge to death was 8.4 months (IQR: 2.0-18.2). In Cox proportional hazards regression models, body mass index (BMI) < 18.5 kg/m2 (adjusted hazard ratio [aHR] = 4.5, 95% confidence interval [CI]: 1.3-15.7), smoking (aHR = 4.7, 95%CI:1.7-13.2), or a clinically significant comorbidity including heart, lung, liver, or renal disorders or auto-immune diseases (aHR = 3.5, 95%CI: 1.3-9.4), were factors independently associated with increased mortality.
Conclusion: Our study suggested an alarming situation of XDR-TB patients in China with a sizable proportion of newly transmitted cases, a high mortality rate, and a long period in community. This observation calls for urgent actions to improve XDR-TB case management in China, including providing regimens with high chances of cure and palliative care, and enhanced infection control measures.
Keywords: Mortality; New case; Risk factors; Survival analysis; Transmission; XDR-TB.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Ethical Review Committee of responsible units (Changsha Central Hospital) and we had received ethics committee approval for verbal consent. We obtained verbal informed consent from all subjects on the phone, if the patient died when we tracked, the verbal consent was received from the legal representative or next of kin of the deceased patients.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- World Health Organization. Global tuberculosis report 2017. WHO/HTM/TB/2017.23. Geneva: World Health Organization. 2017. p. 21–63.
-
- Fan L, Sha W. Long - term prognosis of extensively drug-resistant TB (XDR-TB) in South Africa: a cohort study. Chin J Tuberc Res Dis. 2014;37(10):800.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
