

The Aspirin Regimens in Essential Thrombocythemia (ARES) phase II randomized trial design: Implementation of the serum thromboxane B2 assay as an evaluation tool of different aspirin dosing regimens in the clinical setting
- PMID: 29880847
- PMCID: PMC5992153
- DOI: 10.1038/s41408-018-0078-3
The Aspirin Regimens in Essential Thrombocythemia (ARES) phase II randomized trial design: Implementation of the serum thromboxane B2 assay as an evaluation tool of different aspirin dosing regimens in the clinical setting
Abstract
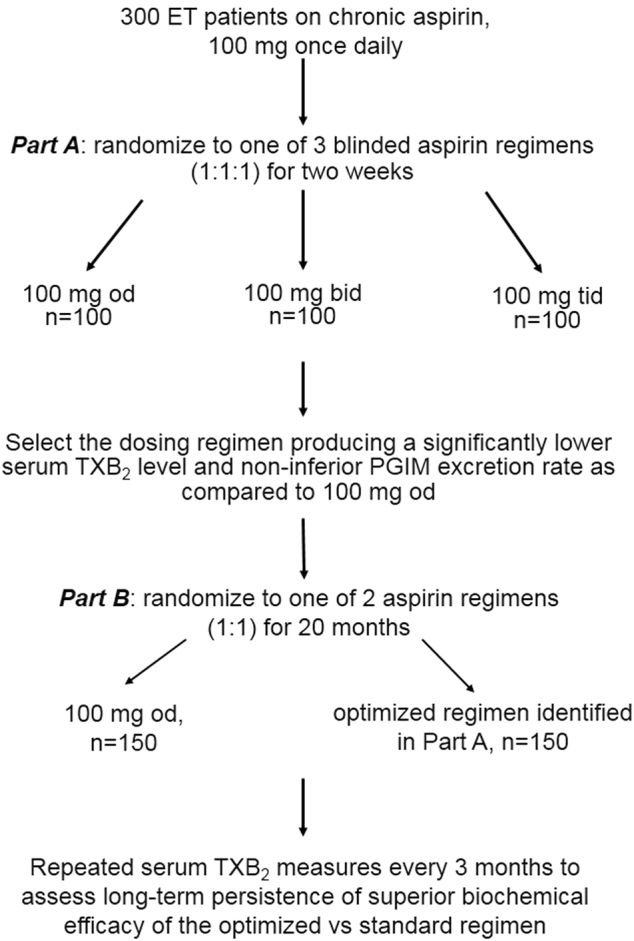
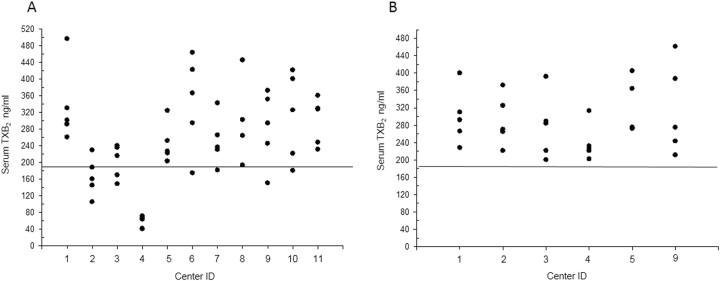
Once-daily (od), low-dose aspirin (75-100 mg) is recommended to reduce the thrombotic risk of patients with essential thrombocytemia (ET). This practice is based on data extrapolated from other high-risk patients and an aspirin trial in polycythemia vera, with the assumption of similar aspirin pharmacodynamics in the two settings. However, the pharmacodynamics of low-dose aspirin is impaired in ET, reflecting accelerated renewal of platelet cyclooxygenase (COX)-1. ARES is a parallel-arm, placebo-controlled, randomized, dose-finding, phase II trial enrolling 300 ET patients to address two main questions. First, whether twice or three times 100 mg aspirin daily dosing is superior to the standard od regimen in inhibiting platelet thromboxane (TX)A2 production, without inhibiting vascular prostacyclin biosynthesis. Second, whether long-term persistence of superior biochemical efficacy can be safely maintained with multiple vs. single dosing aspirin regimen. Considering that the primary study end point is serum TXB2, a surrogate biomarker of clinical efficacy, a preliminary exercise of reproducibility and validation of this biomarker across all the 11 participating centers was implemented. The results of this preliminary phase demonstrate the importance of controlling reproducibility of biomarkers in multicenter trials and the feasibility of using serum TXB2 as a reliable end point for dose-finding studies of novel aspirin regimens.
Conflict of interest statement
V.D.S. has received consulting and lecture fees from Amgen, Bayer, Celgene, Novartis, and institutional research grants from Novartis; B.R. has received consulting and lecture fees from Amgen, Bayer, Celgene, Daiichi Sankyo Italia, Novartis, and Sanofi; A.Ra. has received consulting and lecture fees from Amgen, Bristol Mayer Squibb, Celgene, Italfarmaco, Novartis, Pfizer, and Roche; F.P. has received consulting and lecture fees from Novartis; A.M.V. has received consulting and lecture fees from Italfarmaco, Novartis, Shire, and institutional research grants from Novartis; C.P. has received consulting and lecture fees from Amgen, AstraZeneca, Bayer, and GlaxoSmithKline, and institutional research grants from Bayer; he serves as Chairperson of the Scientific Advisory Board of the International Aspirin Foundation. The remaining authors declare that they have no conflict of interest.
Figures
References
-
- Ryden L, et al. ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD-summary. Diab. Vasc. Dis. Res. 2013;11:133–173. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
