

Unintended Consequences: Fluid Resuscitation Worsens Shock in an Ovine Model of Endotoxemia
- PMID: 29882682
- PMCID: PMC7613331
- DOI: 10.1164/rccm.201801-0064OC
Unintended Consequences: Fluid Resuscitation Worsens Shock in an Ovine Model of Endotoxemia
Abstract
Rationale: Fluid resuscitation is widely considered a life-saving intervention in septic shock; however, recent evidence has brought both its safety and efficacy in sepsis into question.
Objectives: In this study, we sought to compare fluid resuscitation with vasopressors with the use of vasopressors alone in a hyperdynamic model of ovine endotoxemia.
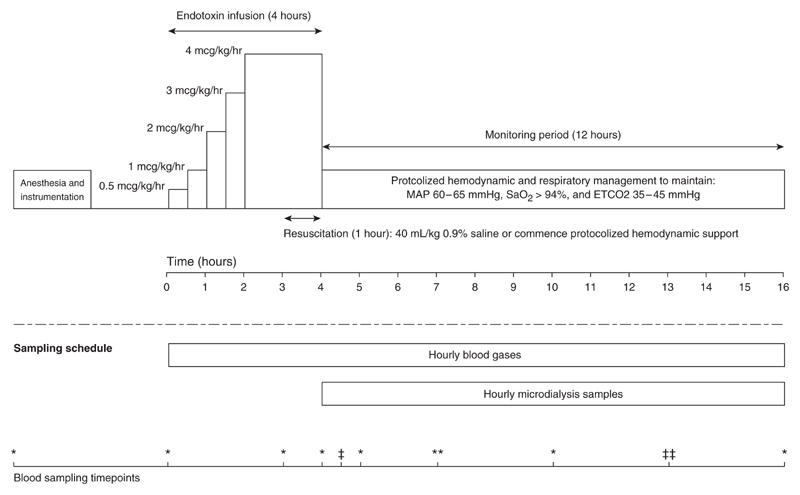
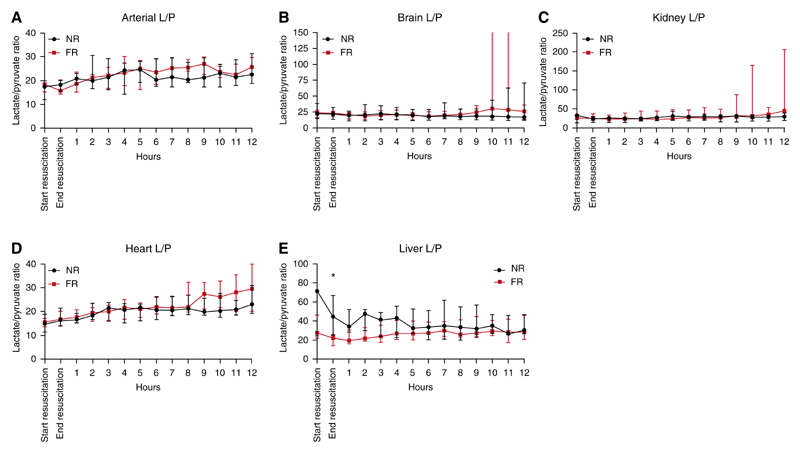
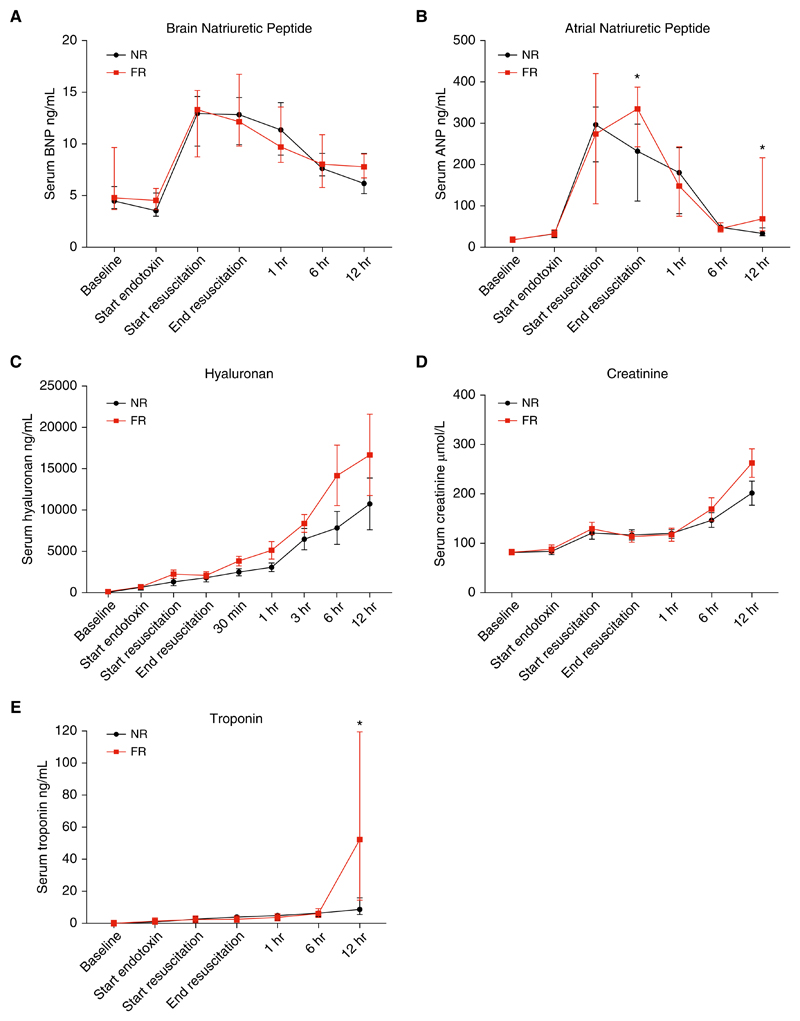
Methods: Endotoxemic shock was induced in 16 sheep, after which they received fluid resuscitation with 40 ml/kg of 0.9% saline or commenced hemodynamic support with protocolized noradrenaline and vasopressin. Microdialysis catheters were inserted into the arterial circulation, heart, brain, kidney, and liver to monitor local metabolism. Blood samples were recovered to measure serum inflammatory cytokines, creatinine, troponin, atrial natriuretic peptide, brain natriuretic peptide, and hyaluronan. All animals were monitored and supported for 12 hours after fluid resuscitation.
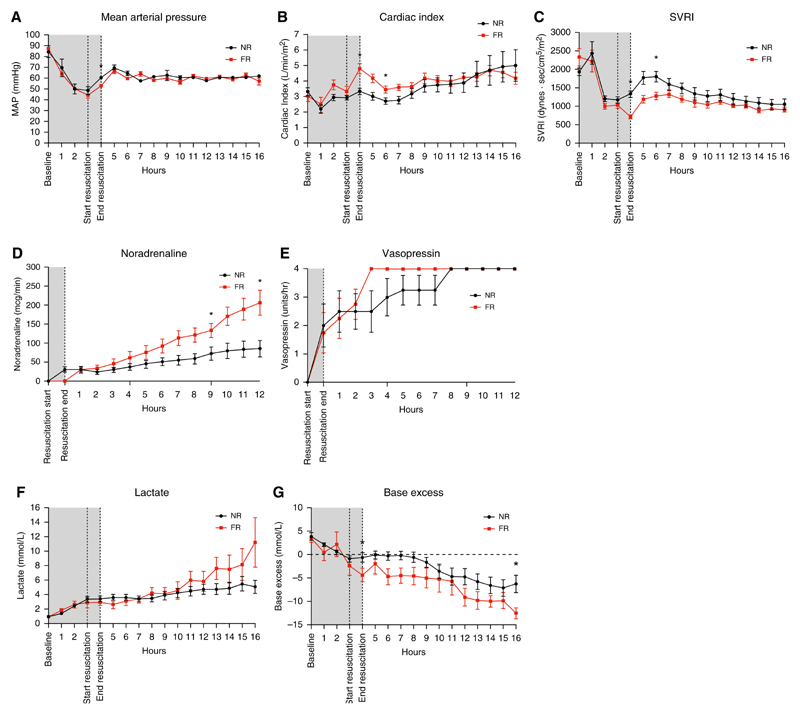
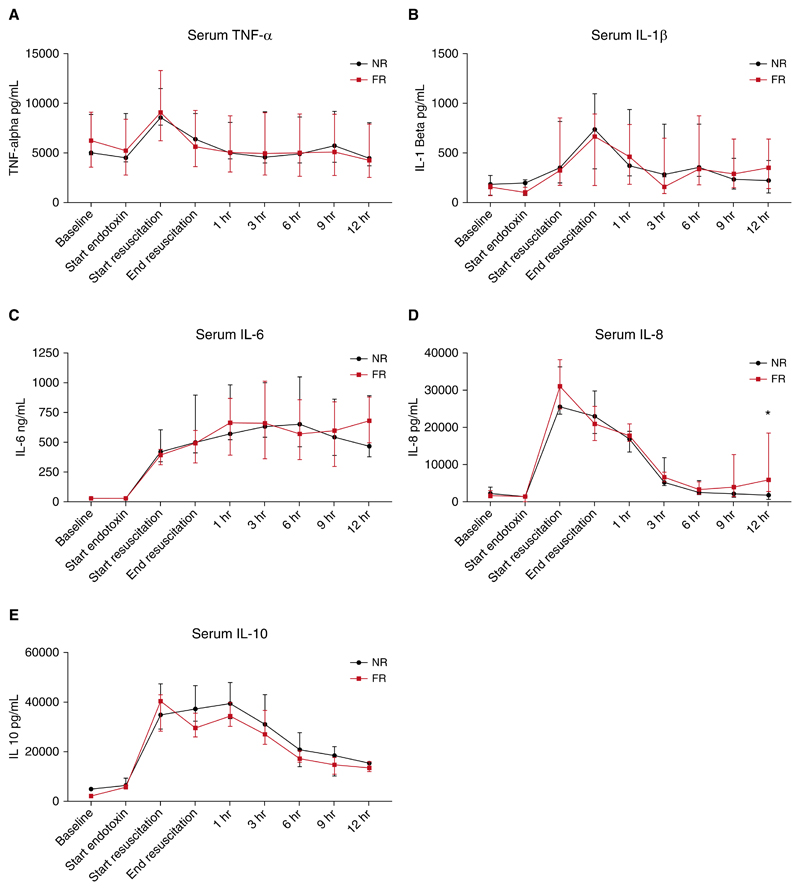
Measurements and main results: After resuscitation, animals that received fluid resuscitation required significantly more noradrenaline to maintain the same mean arterial pressure in the subsequent 12 hours (68.9 mg vs. 39.6 mg; P = 0.04). Serum cytokines were similar between groups. Atrial natriuretic peptide increased significantly after fluid resuscitation compared with that observed in animals managed without fluid resuscitation (335 ng/ml [256-382] vs. 233 ng/ml [144-292]; P = 0.04). Cross-sectional time-series analysis showed that the rate of increase of the glycocalyx glycosaminoglycan hyaluronan was greater in the fluid-resuscitated group over the course of the study (P = 0.02).
Conclusions: Fluid resuscitation resulted in a paradoxical increase in vasopressor requirement. Additionally, it did not result in improvements in any of the measured microcirculatory- or organ-specific markers measured. The increase in vasopressor requirement may have been due to endothelial/glycocalyx damage secondary to atrial natriuretic peptide-mediated glycocalyx shedding.
Keywords: endotoxemia; fluid resuscitation; sepsis; septic shock.
Figures
Comment in
-
Challenging Dogma: The Value of Bolus Fluids in the Early Resuscitation of Hyperdynamic Sepsis.Am J Respir Crit Care Med. 2018 Oct 15;198(8):981-983. doi: 10.1164/rccm.201806-1071ED. Am J Respir Crit Care Med. 2018. PMID: 29940124 No abstract available.
References
-
- Angus DC, van der Poll T. Severe sepsis and septic shock. N Engl J Med. 2013;369:840–851. - PubMed
-
- Hodgin KE, Moss M. The epidemiology of sepsis. CurrPharm Des. 2008;14:1833–1839. - PubMed
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43:304–377. - PubMed
-
- Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, et al. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Intensive Care Med. 2004;30:536–555. - PubMed
