

Dietary Salt Restriction in Chronic Kidney Disease: A Meta-Analysis of Randomized Clinical Trials
- PMID: 29882800
- PMCID: PMC6024651
- DOI: 10.3390/nu10060732
Dietary Salt Restriction in Chronic Kidney Disease: A Meta-Analysis of Randomized Clinical Trials
Abstract
Background: A clear evidence on the benefits of reducing salt in people with chronic kidney disease (CKD) is still lacking. Salt restriction in CKD may allow better control of blood pressure (BP) as shown in a previous systematic review while the effect on proteinuria reduction remains poorly investigated.
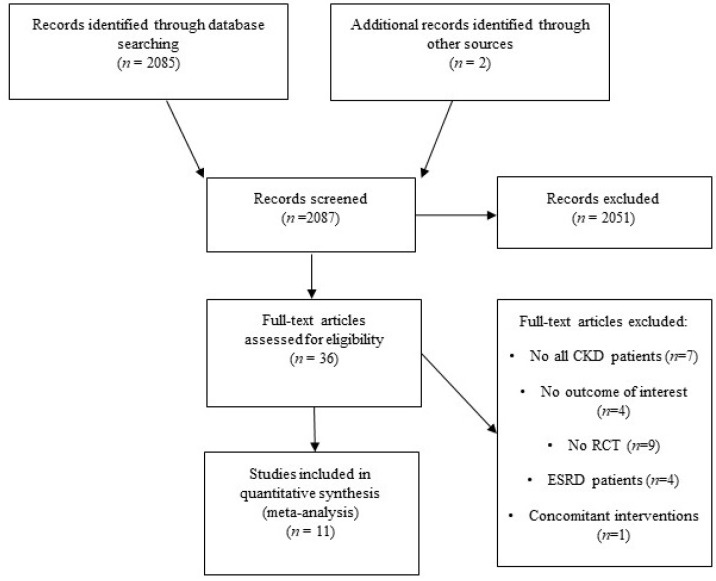
Methods: We performed a meta-analysis of randomized controlled trials (RCTs) evaluating the effects of low versus high salt intake in adult patients with non-dialysis CKD on change in BP, proteinuria and albuminuria.
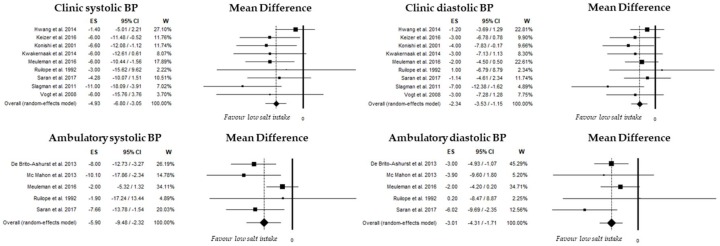
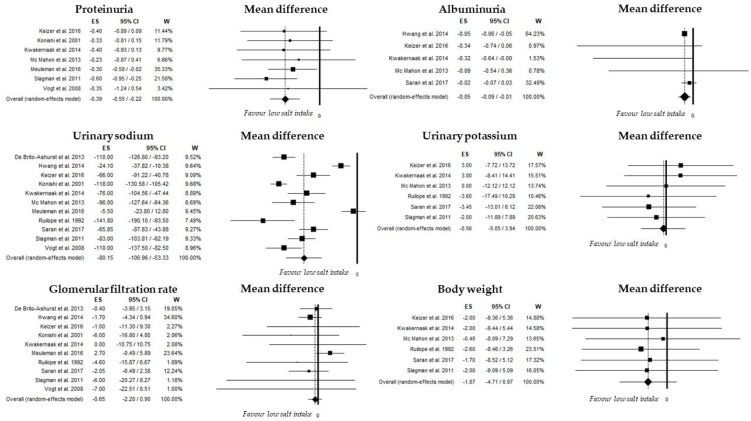
Results: Eleven RCTs were selected and included information about 738 CKD patients (Stage 1⁻4); urinary sodium excretion was 104 mEq/day (95%CI, 76⁻131) and 179 mEq/day (95%CI, 165⁻193) in low- and high-sodium intake subgroups, respectively, with a mean difference of −80 mEq/day (95%CI from −107 to −53; p <0.001). Overall, mean differences in clinic and ambulatory systolic BP were −4.9 mmHg (95%CI from −6.8 to −3.1, p <0.001) and −5.9 mmHg (95%CI from −9.5 to −2.3, p <0.001), respectively, while clinic and ambulatory diastolic BP were −2.3 mmHg (95%CI from −3.5 to −1.2, p <0.001) and −3.0 mmHg (95%CI from −4.3 to −1.7; p <0.001), respectively. Mean differences in proteinuria and albuminuria were −0.39 g/day (95%CI from −0.55 to −0.22, p <0.001) and −0.05 g/day (95%CI from −0.09 to −0.01, p = 0.013).
Conclusion: Moderate salt restriction significantly reduces BP and proteinuria/albuminuria in patients with CKD (Stage 1⁻4).
Keywords: blood pressure; chronic kidney disease; dietary salt restriction; proteinuria.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
