

In-Home Secondhand Smoke Exposure Among Urban Children With Asthma: Contrasting Households With and Without Residential Smokers
- PMID: 29883368
- PMCID: PMC6173659
- DOI: 10.1097/PHH.0000000000000790
In-Home Secondhand Smoke Exposure Among Urban Children With Asthma: Contrasting Households With and Without Residential Smokers
Abstract
Context: Secondhand smoke exposure (SHSe) affects up to half of all children in the United States. Many studies have identified factors associated with in-home SHSe, but few have contrasted these factors between households with and without residential smokers. In the latter case, exposure occurs from only external sources that enter the home, such as visitors or environmental incursion.
Objective: Among children with SHSe at home, to examine demographic and psychosocial differences between households with and without residential smokers.
Design: Baseline analysis of an observational cohort.
Setting: Baltimore City, Maryland.
Participants: A total of 157 children with asthma, aged 5 to 12 years.
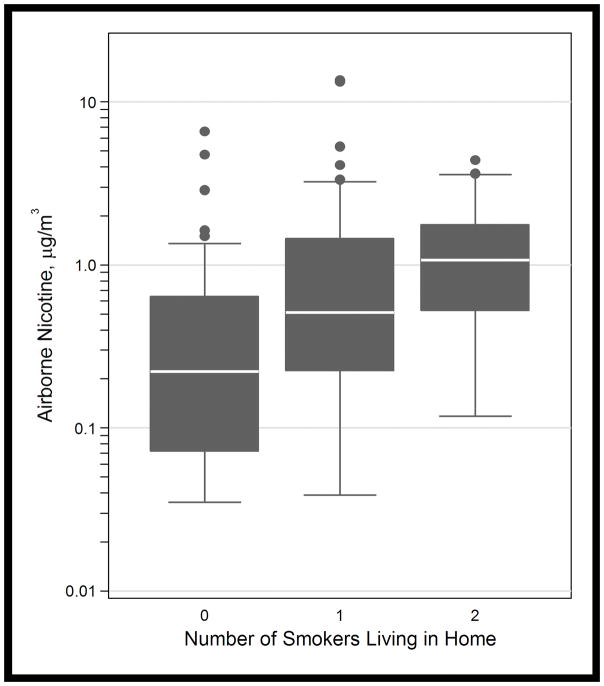
Measures: At-home airborne nicotine, caregiver-reported depression, asthma-related quality of life, functional social support, and demographics. Univariable comparisons were performed between SHS-exposed households with and without residential smokers. Multivariable logistic regression models were fit to examine associations between measured factors and absence of residential smokers.
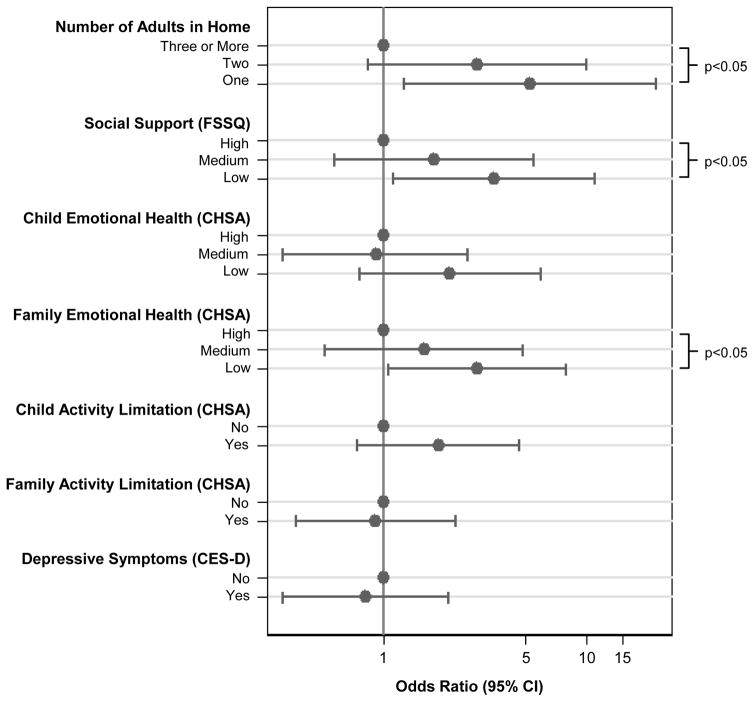
Results: Children (78.3%) had at-home SHSe. Of these, 40.7% lived in households without residential smokers. Compared with households with residential smokers, these caregivers endorsed stronger beliefs in SHS harms and also worse functional social support and asthma-related stress, despite no differences in asthma morbidity. In adjusted models, SHS-exposed children with caregivers in the lowest tertile of functional social support (adjusted odds ratio, 3.50; 95% confidence interval, 1.12-10.99), asthma-related quality of life (2.90; 1.06-7.95), and those living alone (5.28; 1.26-22.15) had at least twice higher odds of having exclusively external SHSe than the highest tertile (P trends < .05).
Conclusions: In-home SHS exposure remains alarmingly high in urban environments. However, a substantial proportion of this exposure appears to be occurring only from external sources that enter the home. Caregivers in these homes had higher desire but lower agency to avoid SHSe, driven by lack of functional support and physical isolation. Public policies targeting these factors may help remediate exposure in this especially vulnerable population.
Figures
Similar articles
-
Factors associated with second-hand smoke exposure in young inner-city children with asthma.J Asthma. 2011 Jun;48(5):449-57. doi: 10.3109/02770903.2011.576742. Epub 2011 May 5. J Asthma. 2011. PMID: 21545248 Free PMC article.
-
Comparison of secondhand smoke exposure in minority and nonminority children with asthma.Health Psychol. 2016 Feb;35(2):115-22. doi: 10.1037/hea0000220. Epub 2015 Aug 3. Health Psychol. 2016. PMID: 26237117 Free PMC article.
-
Provider Counseling About Secondhand Smoke Exposure for Urban Children With Persistent or Poorly Controlled Asthma.J Pediatr Health Care. 2018 Nov-Dec;32(6):612-619. doi: 10.1016/j.pedhc.2018.05.006. Epub 2018 Jul 29. J Pediatr Health Care. 2018. PMID: 30064929 Free PMC article.
-
Assessing secondhand smoke using biological markers.Tob Control. 2013 May;22(3):164-71. doi: 10.1136/tobaccocontrol-2011-050298. Epub 2012 Sep 2. Tob Control. 2013. PMID: 22940677 Free PMC article. Review.
-
The behavioral ecology of secondhand smoke exposure: A pathway to complete tobacco control.Nicotine Tob Res. 2009 Nov;11(11):1254-64. doi: 10.1093/ntr/ntp133. Epub 2009 Sep 23. Nicotine Tob Res. 2009. PMID: 19776346 Free PMC article. Review.
Cited by
-
Short-Term Effects of Side-Stream Smoke on Nerve Growth Factor and Its Receptors TrKA and p75NTR in a Group of Non-Smokers.Int J Environ Res Public Health. 2022 Aug 19;19(16):10317. doi: 10.3390/ijerph191610317. Int J Environ Res Public Health. 2022. PMID: 36011952 Free PMC article.
-
Factors associated with secondhand smoke exposure among non-smoking employees in the workplace: A cross-sectional study in Qingdao, China.PLoS One. 2022 Aug 25;17(8):e0263801. doi: 10.1371/journal.pone.0263801. eCollection 2022. PLoS One. 2022. PMID: 36006979 Free PMC article.
-
The influence of urban exposures and residence on childhood asthma.Pediatr Allergy Immunol. 2022 May;33(5):e13784. doi: 10.1111/pai.13784. Pediatr Allergy Immunol. 2022. PMID: 35616896 Free PMC article. Review.
References
-
- Quinto K, Kit B, Lukacs S, Akinbami L. Environmental tobacco smoke exposure in children aged 3–19 years with and without asthma in the United States, 1999–2010. National Center for Health Statistics; 2013. - PubMed
-
- U.S. Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General. U.S. Department of Health and Human Services, Center for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2006.
-
- Wang Z, May SM, Charoenlap S, et al. Effects of secondhand smoke exposure on asthma morbidity and health care utilization in children: a systematic review and meta-analysis. Ann Allergy Asthma Immunol. 2015;115(5):396–401. e392. - PubMed
-
- Jin Y, Seiber EE, Ferketich AK. Secondhand smoke and asthma: what are the effects on healthcare utilization among children? Prev Med. 2013;57(2):125–128. - PubMed
-
- Hopper JA, Craig KA. Environmental tobacco smoke exposure among urban children. Pediatrics. 2000;106(4):E47. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
