

Is body mass index associated with outcomes of mechanically ventilated adult patients in intensive critical units? A systematic review and meta-analysis
- PMID: 29883469
- PMCID: PMC5993298
- DOI: 10.1371/journal.pone.0198669
Is body mass index associated with outcomes of mechanically ventilated adult patients in intensive critical units? A systematic review and meta-analysis
Abstract
Background: Obesity paradox refers to lower mortality in subjects with higher body mass index (BMI), and has been documented under a variety of condition. However, whether obesity paradox exists in adults requiring mechanical ventilation in intensive critical units (ICU) remains controversial.
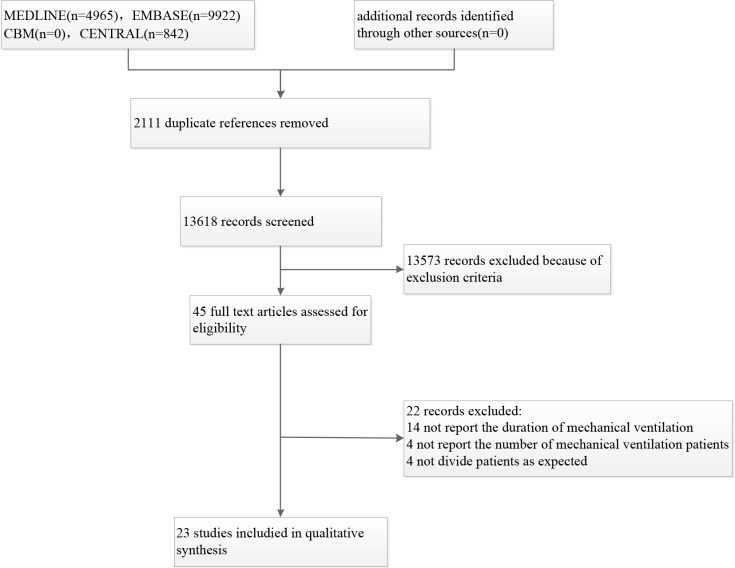
Methods: MEDLINE, EMBASE, China Biology Medicine disc (CBM) and CINAHL electronic databases were searched from the earliest available date to July 2017, using the following search terms: "body weight", "body mass index", "overweight" or "obesity" and "ventilator", "mechanically ventilated", "mechanical ventilation", without language restriction. Subjects were divided into the following categories based on BMI (kg/m2): underweight, < 18.5 kg/m2; normal, 18.5-24.9 kg/m2; overweight, BMI 25-29.9 kg/m2; obese, 30-39.9 kg/m2; and severely obese > 40 kg/m2. The primary outcome was mortality, and included ICU mortality, hospital mortality, short-term mortality (<6 months), and long-term mortality (6 months or beyond). Secondary outcomes included duration of mechanical ventilation, length of stay (LOS) in ICU and hospital. A random-effects model was used for data analyses. Risk of bias was assessed using the Newcastle-Ottawa quality assessment scale.
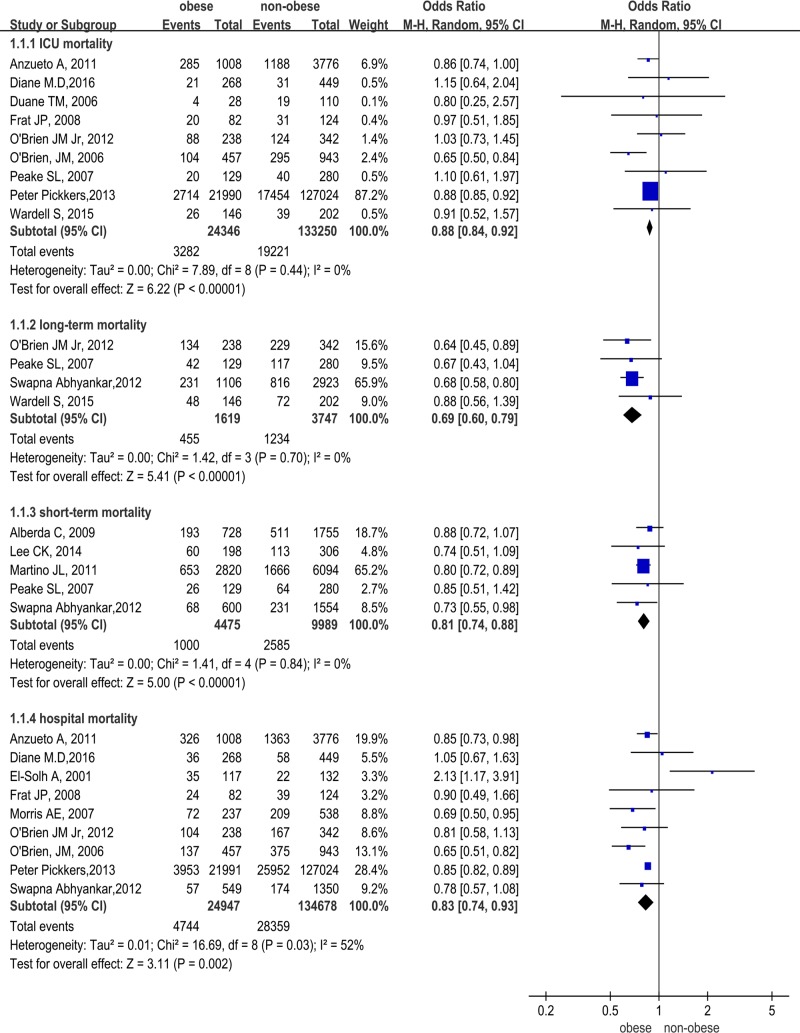
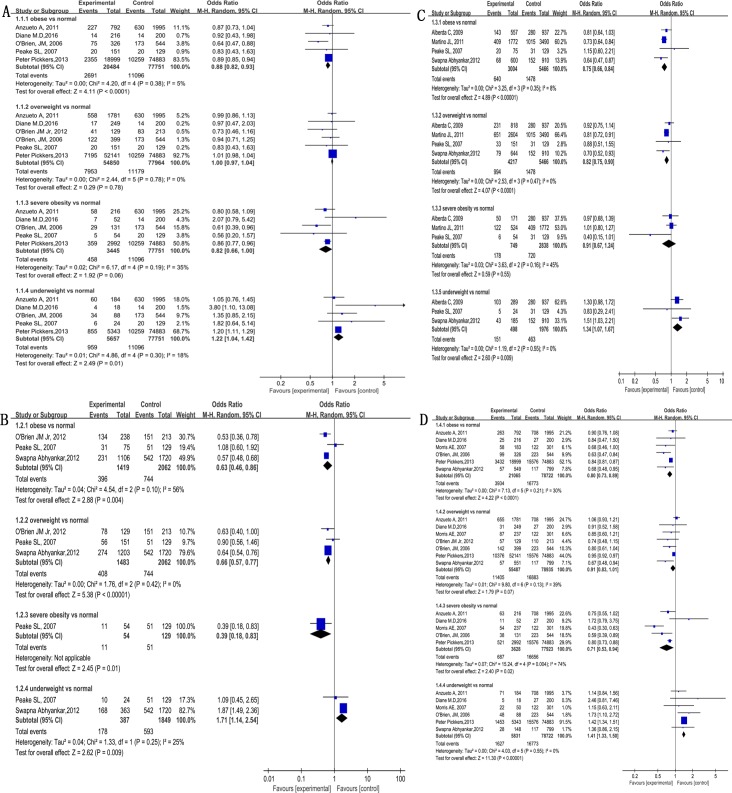
Results: A total of 15,729 articles were screened. The final analysis included 23 articles (199,421 subjects). In comparison to non-obese patients, obese patients had lower ICU mortality (odds ratio (OR) 0.88, 95% CI 0.0.84-0.92, I2 = 0%), hospital mortality (OR 0.83, 95% CI 0.74-0.93, I2 = 52%), short-term mortality (OR 0.81, 95% CI 0.74-0.88, I2 = 0%) as well as long-term mortality (OR 0.69, 95% CI 0.60-0.79, I2 = 0%). In comparison to subjects with normal BMI, obese patients had lower ICU mortality (OR 0.88, 95% CI 0.82-0.93, I2 = 5%). Hospital mortality was lower in severely obese and obese subjects (OR 0.71, 95% CI 0.53-0.94, I2 = 74%, and OR 0.80, 95% CI 0.73-0.89, I2 = 30%). Short-term mortality was lower in overweight and obese subjects (OR 0.82, 95% CI 0.75-0.90, I2 = 0%, and, OR 0.75, 95% CI 0.66-0.84, I2 = 8%, respectively). Long-term mortality was lower in severely obese, obese and overweight subjects (OR 0.39, 95% CI 0.18-0.83, and OR 0.63, 95% CI 0.46-0.86, I2 = 56%, and OR 0.66, 95% CI 0.57-0.77, I2 = 0%). All 4 mortality measures were higher in underweight subjects than in subjects with normal BMI. Obese subjects had significantly longer duration on mechanical ventilation than non-obese group (mean difference (MD) 0.48, 95% CI 0.16-0.80, I2 = 37%), In comparison to subjects with normal BMI, severely obese BMI had significantly longer time in mechanical ventilation (MD 1.10, 95% CI 0.38-1.83, I2 = 47%). Hospital LOS did not differ between obese and non-obese patients (MD 0.05, 95% CI -0.52 to 0.50, I2 = 80%). Obese patients had longer ICU LOS than non-obese patients (MD 0.38, 95% CI 0.17-0.59, I2 = 70%). Hospital LOS and ICU LOS did not differ significantly in subjects with different BMI status.
Conclusions: In ICU patients receiving mechanical ventilation, higher BMI is associated with lower mortality and longer duration on mechanical ventilation.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Prevalence of obesity and the effect on length of mechanical ventilation and length of stay in intensive care patients: A single site observational study.Aust Crit Care. 2017 May;30(3):145-150. doi: 10.1016/j.aucc.2016.07.003. Epub 2016 Aug 10. Aust Crit Care. 2017. PMID: 27522470
-
Increased body mass index and adjusted mortality in ICU patients with sepsis or septic shock: a systematic review and meta-analysis.Crit Care. 2016 Jun 15;20(1):181. doi: 10.1186/s13054-016-1360-z. Crit Care. 2016. PMID: 27306751 Free PMC article.
-
Can body mass index predict clinical outcomes for patients with acute lung injury/acute respiratory distress syndrome? A meta-analysis.Crit Care. 2017 Feb 22;21(1):36. doi: 10.1186/s13054-017-1615-3. Crit Care. 2017. PMID: 28222804 Free PMC article. Review.
-
Early mobilization of trauma patients admitted to intensive care units: A systematic review and meta-analyses.Injury. 2019 Nov;50(11):1809-1815. doi: 10.1016/j.injury.2019.09.007. Epub 2019 Sep 9. Injury. 2019. PMID: 31526602
-
Impact of body mass index on outcomes following critical care.Chest. 2003 Apr;123(4):1202-7. doi: 10.1378/chest.123.4.1202. Chest. 2003. PMID: 12684312
Cited by
-
Extracellular vesicle therapeutics from plasma and adipose tissue.Nano Today. 2021 Aug;39:101159. doi: 10.1016/j.nantod.2021.101159. Epub 2021 Apr 27. Nano Today. 2021. PMID: 33968157 Free PMC article.
-
A nomogram to predict prolonged stay of obesity patients with sepsis in ICU: Relevancy for predictive, personalized, preventive, and participatory healthcare strategies.Front Public Health. 2022 Aug 11;10:944790. doi: 10.3389/fpubh.2022.944790. eCollection 2022. Front Public Health. 2022. PMID: 36033731 Free PMC article. Clinical Trial.
-
Should We Perform Old-for-Old Kidney Transplantation during the COVID-19 Pandemic? The Risk for Post-Operative Intensive Stay.J Clin Med. 2020 Jun 12;9(6):1835. doi: 10.3390/jcm9061835. J Clin Med. 2020. PMID: 32545566 Free PMC article.
-
Epidemiology and outcomes of obese critically ill patients in Australia and New Zealand.Crit Care Resusc. 2020 Mar;22(1):35-44. doi: 10.51893/2020.1.oa4. Crit Care Resusc. 2020. PMID: 32102641 Free PMC article.
-
Association Between Obesity and Short-And Long-Term Mortality in Patients With Acute Respiratory Distress Syndrome Based on the Berlin Definition.Front Endocrinol (Lausanne). 2021 Feb 12;11:611435. doi: 10.3389/fendo.2020.611435. eCollection 2020. Front Endocrinol (Lausanne). 2021. PMID: 33643222 Free PMC article.
References
-
- Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL.Trends in Obesity Among Adults in the United States, 2005 to 2014. Jama. 2016;315(21):2284 doi: 10.1001/jama.2016.6458 . - DOI - PMC - PubMed
-
- Arabi YM, Dara SI, Tamim HM, Rishu AH, Bouchama A, Khedr MK, et al. Clinical characteristics, sepsis interventions and outcomes in the obese patients with septic shock: an international multicenter cohort study. Crit Care. 2013;17(2):R72 doi: 10.1186/cc12680 . - DOI - PMC - PubMed
-
- Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:1–253. . - PubMed
-
- Wang S, Ma W, Wang S, Yi X, Jia H, Xue F. Obesity and Its Relationship with Hypertension among Adults 50 Years and Older in Jinan, China. Plos One. 2014;9(12):e114424 doi: 10.1371/journal.pone.0114424 . - DOI - PMC - PubMed
-
- Gortmaker SL, Swinburn BA, Levy D, Carter R, Mabry PL, Finegood DT, et al. Changing the future of obesity: science, policy, and action. The Lancet. 2011;378(9793):838–847. doi: 10.1016/S0140-6736(11)60815-5 . - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
