

Oral manifestation of Langerhans cell histiocytosis: a case report
- PMID: 29884166
- PMCID: PMC5994067
- DOI: 10.1186/s12903-018-0568-5
Oral manifestation of Langerhans cell histiocytosis: a case report
Abstract
Background: Bone necrosis of the jaw is a serious condition with a broad differential diagnosis of pathologies such as cutaneous histiocytosis, bone metastases or malignant tumours. In addition to the most common cause, medication related osteonecrosis of the jaw (MRONJ), one must consider a number of other causes, such as histiocytosis. Langerhans cell histiocytosis (LCH) is a histiocytic disorder with a large spectrum of clinical manifestations and with possible involvement of a variety of organs. This case shows the importance of an early detection of this rare disease in order to prevent further spreading. Even if an initial diagnosis in the oral cavity is rare, dentists should be aware of this disease.
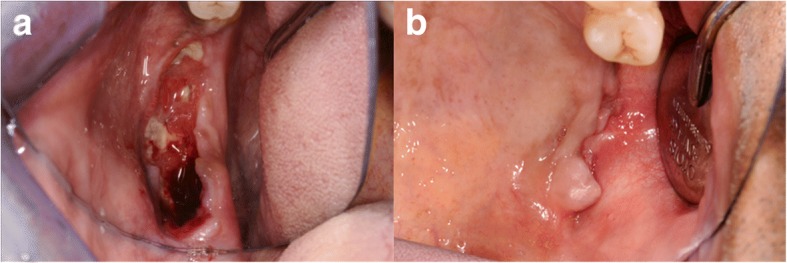
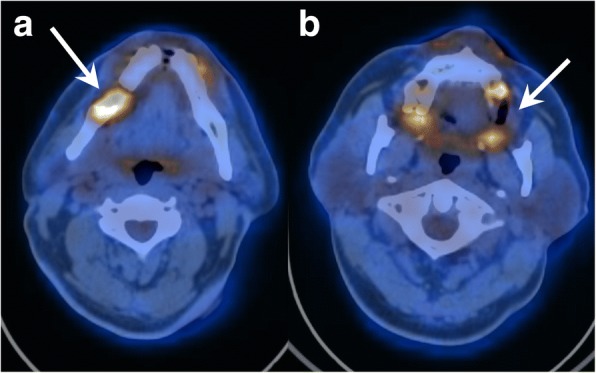
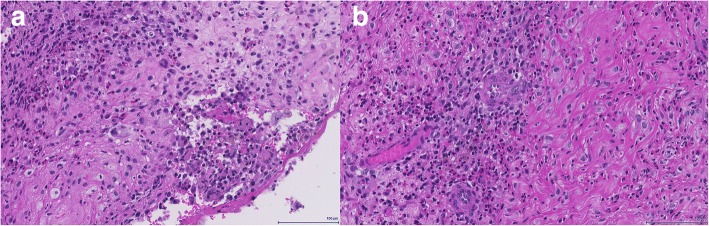
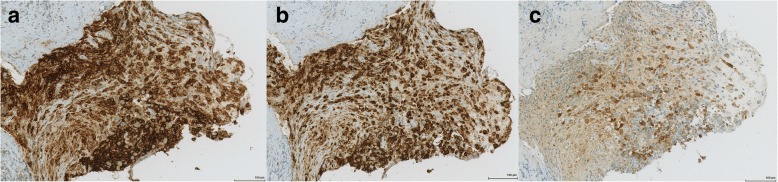
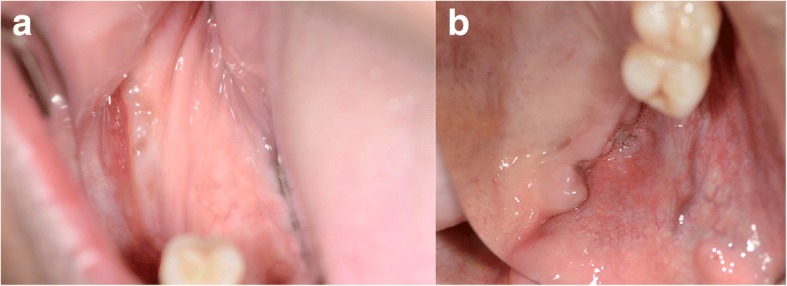
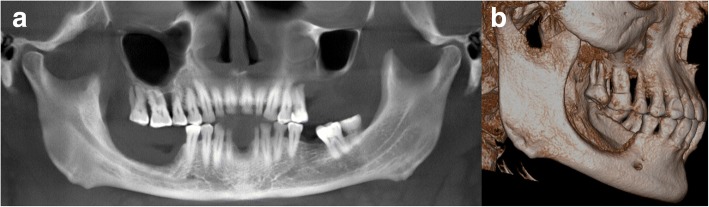
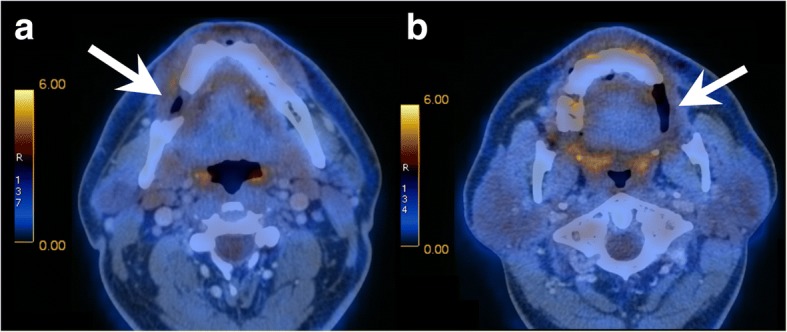
Case presentation: The presented case describes a patient who was referred for evaluation and treatment due to exposed bone and extensive osteolysis in the region of the upper and lower jaw. After biopsy and diagnosis of LCH, the patient was treated with systemic therapy, achieved remission and is disease free after a 2 year of follow up.
Conclusions: This case report illustrates that when dealing with unclear osteolytic changes of the jawbone, Langerhans cell histiocytosis must be taken into consideration in the differential diagnosis and biopsy must be performed in case of suspicion.
Keywords: Eosinophilic granuloma; Histiocytosis; Langerhans-cell; Osteonecrosis.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
The patient signed an approval for the publication of a case report under anonymized conditions.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Allen CE, Li L, Peters TL, Leung HC, Yu A, Man TK, Gurusiddappa S, Phillips MT, Hicks MJ, Gaikwad A, et al. Cell-specific gene expression in Langerhans cell histiocytosis lesions reveals a distinct profile compared with epidermal Langerhans cells. J Immunol. 2010;184(8):4557–4567. doi: 10.4049/jimmunol.0902336. - DOI - PMC - PubMed
-
- Emile JF, Abla O, Fraitag S, Horne A, Haroche J, Donadieu J, Requena-Caballero L, Jordan MB, Abdel-Wahab O, Allen CE, et al. Revised classification of histiocytoses and neoplasms of the macrophage-dendritic cell lineages. Blood. 2016;127(22):2672–2681. doi: 10.1182/blood-2016-01-690636. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
