

Neurologic outcomes in pediatric cardiac arrest survivors enrolled in the THAPCA trials
- PMID: 29884735
- PMCID: PMC6053110
- DOI: 10.1212/WNL.0000000000005773
Neurologic outcomes in pediatric cardiac arrest survivors enrolled in the THAPCA trials
Abstract
Objective: To implement a standardized approach to characterize neurologic outcomes among 12-month survivors in the Therapeutic Hypothermia after Pediatric Cardiac Arrest (THAPCA) trials.
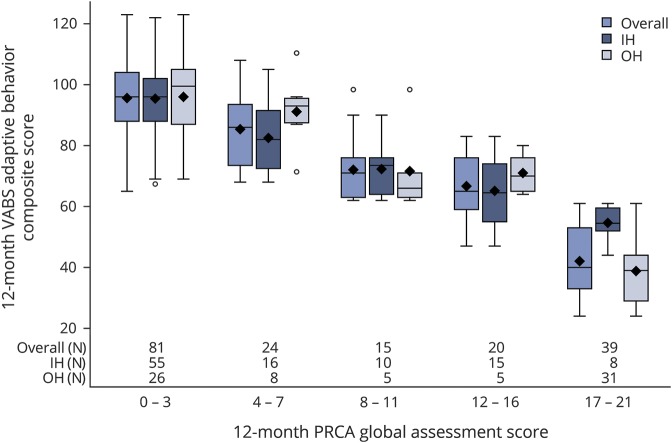
Methods: Two multicenter trials enrolled children age 48 hours to 18 years who remained comatose after cardiac arrest (CA) occurring out-of-hospital (THAPCA-OH, NCT00878644) or in-hospital (THAPCA-IH, NCT00880087); patients were randomized to therapeutic hypothermia or therapeutic normothermia. The primary outcome, survival with favorable 12-month neurobehavioral outcome (Vineland Adaptive Behavior Scales [VABS-II]), did not differ between treatment groups in either trial. Neurologists examined 181 12-month survivors, described findings using the novel semi-quantitative Pediatric Resuscitation after Cardiac Arrest (PRCA) form, and rated findings in 6 domains; scores ranged from 0 (no deficits) to 21 (maximal deficits). PRCA scores were compared with 12-month VABS-II scores and cognitive scores.
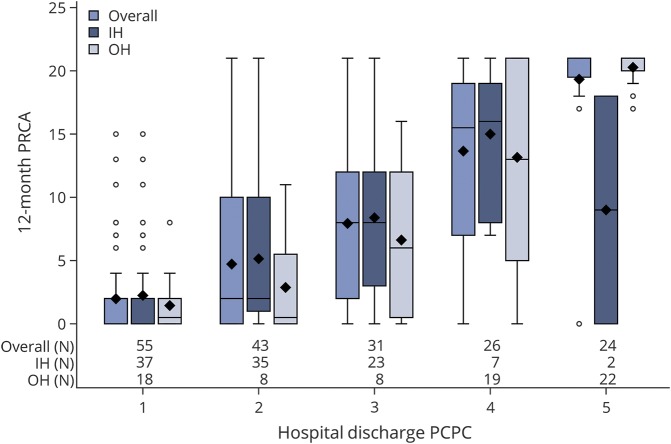
Results: Neurologic outcome PRCA scores were classified as no/minimal impairment, PRCA 0-3, 81/179 (45%); mild impairment, PRCA 4-7, 24/179 (13%); moderate impairment, PRCA 8-11, 15/179 (8%); severe impairment, PRCA 12-16, 20/179 (11%); profound impairment, PRCA 17-21, 39/179 (21%) (2/181 incomplete). VABS-II scores correlated strongly with PRCA category (r = -0.88, p < 0.0001, Pearson correlation coefficient) and cognitive scores (r = -0.72, p < 0.0001). Factors associated with poor outcomes included out-of-hospital CA, seizure recognition in the early postarrest period, and poor neurologic status at hospital discharge.
Conclusion: The PRCA provides a robust method for depicting neurologic outcomes after acute encephalopathy caused by CA in children. It provides a global semiquantitative rating of neurologic impairment and domain-specific impairment. The strong correlation with well-established neurobehavioral outcome measures supports its validity over a broad age range and wide spectrum of outcomes.
© 2018 American Academy of Neurology.
Figures
References
-
- Kitchen L, Westmacott R, Friefeld S, et al. . The Pediatric Stroke Outcome Measure: a validation and reliability study. Stroke 2012;43:1602–1608. - PubMed
-
- Sparrow SCD, Balla D. Vineland Adaptive Behavior Scales: Survey Forms Manual. 2nd ed. Minneapolis: NCS Pearson; 2005.
-
- Fiser DH, Long N, Roberson PK, Hefley G, Zolten K, Brodie-Fowler M. Relationship of pediatric overall performance category and Pediatric Cerebral Performance Category scores at pediatric intensive care unit discharge with outcome measures collected at hospital discharge and 1- and 6-month follow-up assessments. Crit Care Med 2000;28:2616–2620. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical