

β-Cell secretory defects are present in pancreatic insufficient cystic fibrosis with 1-hour oral glucose tolerance test glucose ≥155 mg/dL
- PMID: 29885044
- PMCID: PMC6364976
- DOI: 10.1111/pedi.12700
β-Cell secretory defects are present in pancreatic insufficient cystic fibrosis with 1-hour oral glucose tolerance test glucose ≥155 mg/dL
Abstract
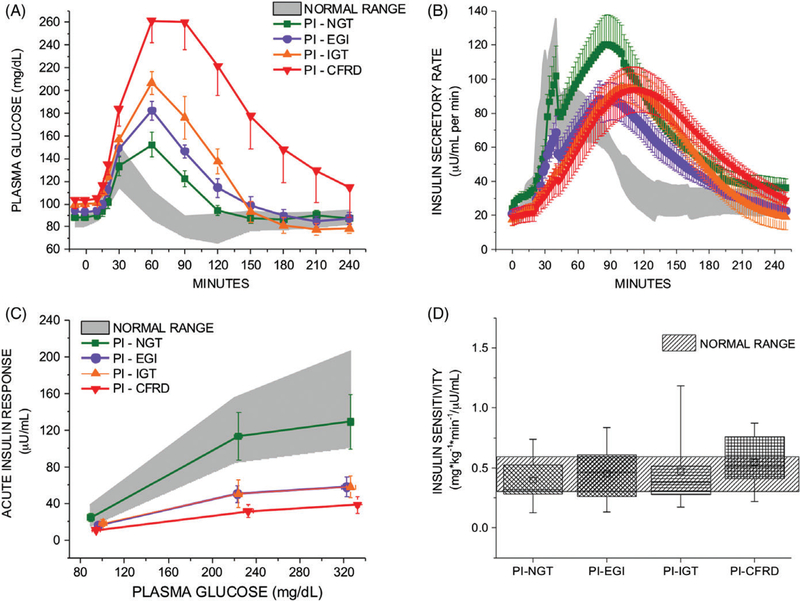
Background: Patients with pancreatic insufficient cystic fibrosis (PI-CF) meeting standard criteria for normal glucose tolerance display impaired β-cell secretory capacity and early-phase insulin secretion defects. We sought evidence of impaired β-cell secretory capacity, a measure of functional β-cell mass, among those with early glucose intolerance (EGI), defined as 1-hour oral glucose tolerance test (OGTT) glucose ≥155 mg/dL (8.6 mmol/L).
Methods: A cross-sectional study was conducted in the Penn and CHOP Clinical & Translational Research Centers. PI-CF categorized by OGTT as normal (PI-NGT: 1-hour glucose <155 mg/dL and 2-hour <140 mg/dL [7.8 mmol/L]; n = 13), PI-EGI (1-hour ≥155 mg/dL and 2-hour <140 mg/dL; n = 13), impaired (PI-IGT: 2-hour ≥140 and <200 mg/dL [11.1 mmol/L]; n = 8), and diabetic (cystic fibrosis-related diabetes, CFRD: 2-hour ≥200 mg/dL; n = 8) participated. Post-prandial glucose tolerance and insulin secretion, and β-cell secretory capacity and demand were derived from mixed-meal tolerance tests (MMTTs), and glucose-potentiated arginine (GPA) tests, respectively.
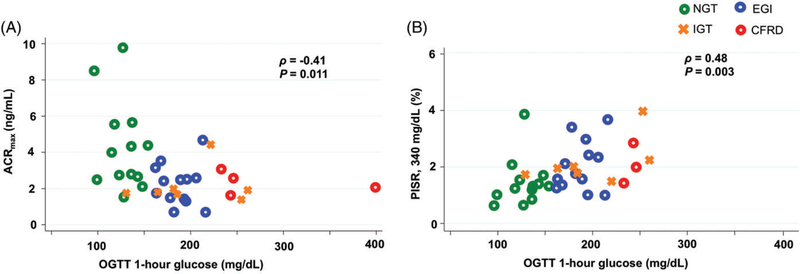
Results: PI-EGI had elevated post-prandial glucose with reduced early-phase insulin secretion during MMTT compared to PI-NGT (P < .05). PI-EGI also exhibited impaired acute insulin and C-peptide responses to GPA (P < .01 vs PI-NGT), measures of β-cell secretory capacity. Proinsulin secretory ratios were higher under hyperglycemic clamp conditions in PI-IGT and CFRD (P < .05 vs PI-NGT), and correlated with 1-hour glucose in PI-CF (P < .01).
Conclusions: PI-CF patients with 1-hour OGTT glucose ≥155 mg/dL already manifest impaired β-cell secretory capacity with associated early-phase insulin secretion defects. Avoiding hyperglycemia in patients with EGI may be important for preventing excessive insulin demand indicated by disproportionately increased proinsulin secretion.
Keywords: cystic fibrosis-related diabetes; early glucose intolerance; insulin secretion; proinsulin secretory ratio; β-cell secretory capacity.
© 2018 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Conflict of interest statement
Conflict of interest
No potential conflicts of interest relevant to this article exist and all authors have reviewed and approved submission of this manuscript.
Figures
References
-
- Marshall BC, Butler SM, Stoddard M, Moran AM, Liou TG, Morgan WJ. Epidemiology of cystic fibrosis-related diabetes. J Pediatr 2005;146(5):681–687. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
