

Transcranial direct current brain stimulation decreases impulsivity in ADHD
- PMID: 29885858
- PMCID: PMC6109423
- DOI: 10.1016/j.brs.2018.04.016
Transcranial direct current brain stimulation decreases impulsivity in ADHD
Abstract
Background: Impulsivity is a core deficit in attention deficit hyperactivity disorder (ADHD). Transcranial direct current stimulation (tDCS) of the dorsolateral prefrontal cortex (DLPFC) has been shown to modulate cognitive control circuits and could enhance DLPFC activity, leading to improved impulse control in ADHD.
Objective: Hypothesis: We predicted 2.0 mA anodal stimulation (tDCS) versus sham stimulation applied over the left DLPFC would improve Conners Continuous Performance Task (CPT) scores. Our secondary hypothesis predicted that stop signal task (SST) reaction time (SSRT) would decrease with tDCS (versus sham).
Methods: Thirty-seven participants completed two periods of three tDCS (or sham) sessions two weeks apart in a within-subject, double-blind, counterbalanced order. Participants performed a fractal N-back training task concurrent with tDCS (or sham) stimulation. Participants completed the CPT and SST at the beginning of treatment (baseline), at the end of the treatment, and at a 3-day post-stimulation follow-up.
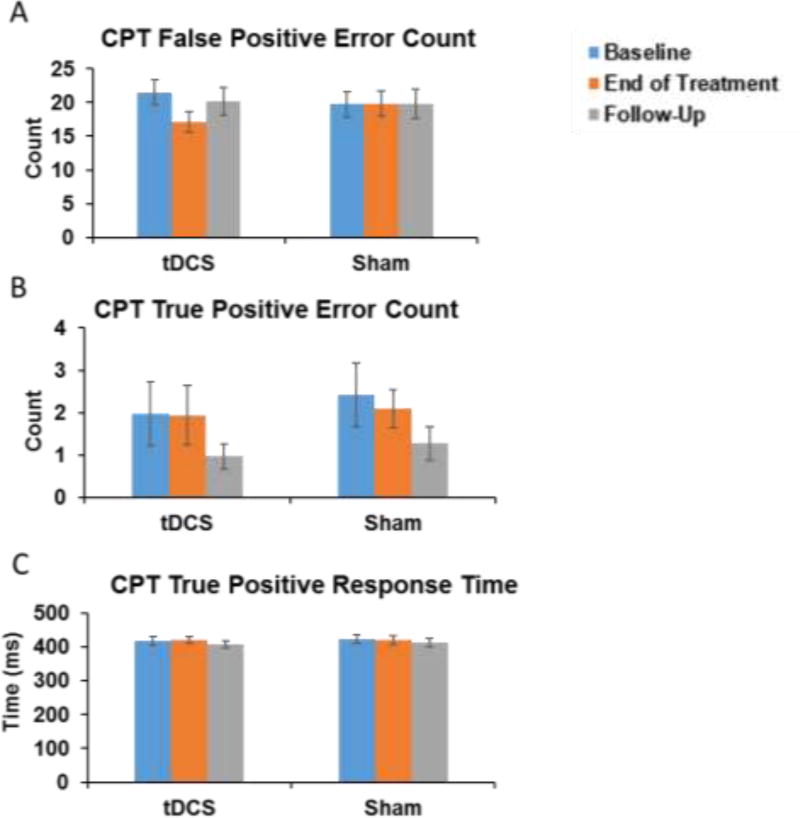
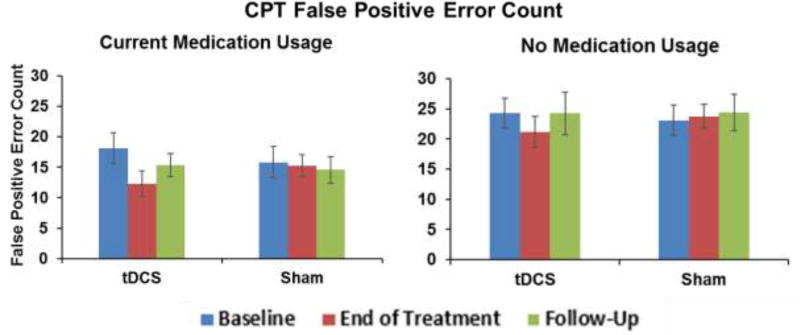
Results: There was a significant stimulation condition by session interaction for CPT false positive scores (χ2 = 15.44, p < 0.001) driven by a decrease in false positive errors from baseline to end of treatment in the tDCS group (β = -0.36, 95% Confidence Interval (CI) -0.54 to -0.18, p < 0.001). This effect did not persist at follow-up (β = -0.13, p > 0.05). There was no significant stimulation condition by session interaction effect on CPT true positive errors or response time (ps > 0.05). No significant change in SSRT performance was observed (p > 0.05).
Conclusion: These findings suggest that stimulation of the left DLPFC with tDCS can improve impulsivity symptoms in ADHD, supporting the therapeutic potential for tDCS in adult ADHD patients.
Keywords: Attention deficit hyperactivity disorder; Continuous performance task; Dorsolateral prefrontal cortex; Impulsivity; tDCS.
Copyright © 2018. Published by Elsevier Inc.
Conflict of interest statement
None
Figures
References
-
- Sharma A, Couture J. A review of the pathophysiology, etiology, and treatment of attention-deficit hyperactivity disorder (ADHD) Ann Pharmacother. 2014;48(2):209–25. - PubMed
-
- Lensing MB, Zeiner P, Sandvik L, Opjordsmoen S. Four-year outcome in psychopharmacologically treated adults with attention-deficit/hyperactivity disorder: a questionnaire survey. J Clin Psychiatry. 2013;74(1):e87–93. - PubMed
-
- Spencer T, Biederman J, Wilens T. Pharmacotherapy of attention deficit hyperactivity disorder. Child Adolesc Psychiatr Clin N Am. 2000;9(1):77–97. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
