

Self-Rated Health Status and Risk of Incident Stroke in 0.5 Million Chinese Adults: The China Kadoorie Biobank Study
- PMID: 29886721
- PMCID: PMC6007294
- DOI: 10.5853/jos.2017.01732
Self-Rated Health Status and Risk of Incident Stroke in 0.5 Million Chinese Adults: The China Kadoorie Biobank Study
Abstract
Background and purpose: Self-rated health (SRH) is a consistent and strong predictor of all-cause and cardiovascular mortality in various populations. However, the associations between SRH measures and risk of first-ever or recurrent stroke were rarely explored. We thus aim to prospectively investigate the associations between SRH measures and risk of total and subtypes of stroke in Chinese population.
Methods: A total of 494,113 participants from the China Kadoorie Biobank without prior heart diseases or cancer (486,541 without stroke and 7,572 with stroke) were followed from baseline (2004 to 2008) until December 31, 2013. General and age-comparative SRH were obtained from baseline questionnaires. First-ever stroke or recurrent events were ascertained through linkage to disease registry system and health insurance data.
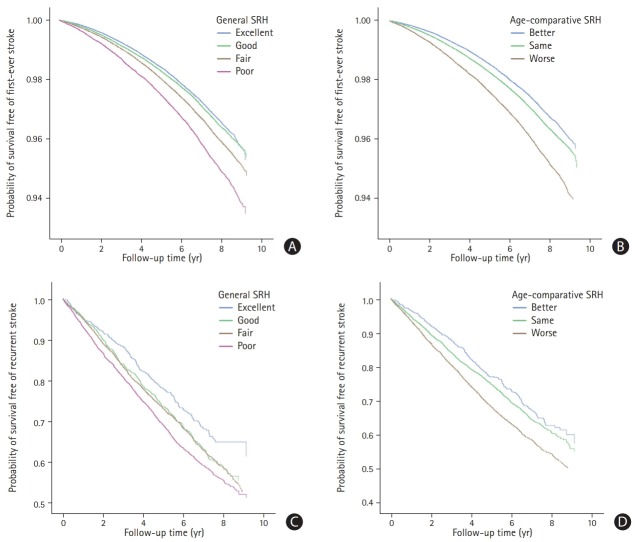
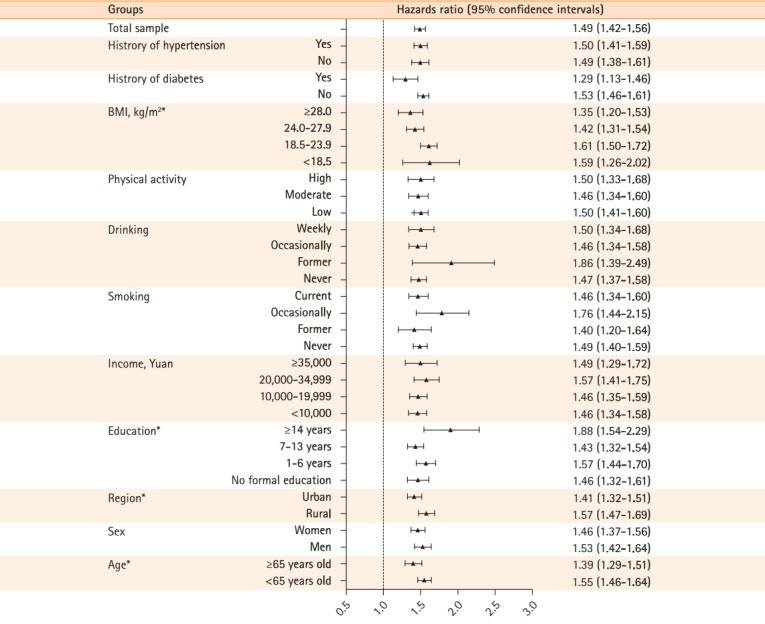
Results: We identified 27,662 first-ever stroke and 2,909 recurrent events during an average of 7.0 years of follow-up. Compared with excellent general SRH, the hazard ratios (HRs) and 95% confidence intervals (CIs) for first-ever stroke associated with good, fair, and poor general SRH were 1.04 (1.00 to 1.08), 1.19 (1.15 to 1.23), and 1.49 (1.42 to 1.56) in the multivariate model, respectively. Compared with better age-comparative SRH, the HRs (95% CIs) of same and worse age-comparative SRH were 1.13 (1.10 to 1.17) and 1.51 (1.45 to 1.58), respectively. The relations of SRH measures with ischemic stroke, hemorrhagic stroke, and recurrent stroke were similar to that with total first-ever stroke. However, the magnitude of associations was much stronger for fatal stroke than for non-fatal stroke.
Conclusions: This large-scale prospective cohort suggests that self-perceived health status is associated with incident stroke, regardless of stroke subtype.
Keywords: Health status; Prospective studies; Stroke.
Figures
Similar articles
-
Self-rated health after stroke: a systematic review of the literature.BMC Neurol. 2019 Sep 7;19(1):221. doi: 10.1186/s12883-019-1448-6. BMC Neurol. 2019. PMID: 31493791 Free PMC article.
-
Self-Rated Health Status and Risk of Ischemic Heart Disease in the China Kadoorie Biobank Study: A Population-Based Cohort Study.J Am Heart Assoc. 2017 Sep 22;6(9):e006595. doi: 10.1161/JAHA.117.006595. J Am Heart Assoc. 2017. PMID: 28939702 Free PMC article.
-
Association between multiple comorbidities and self-rated health status in middle-aged and elderly Chinese: the China Kadoorie Biobank study.BMC Public Health. 2018 Jun 15;18(1):744. doi: 10.1186/s12889-018-5632-1. BMC Public Health. 2018. PMID: 29907132 Free PMC article.
-
[Self-rated health measures and their relations to all-cause and cardiovascular mortality in adults from 10 regions of China].Zhonghua Liu Xing Bing Xue Za Zhi. 2021 May 10;42(5):763-770. doi: 10.3760/cma.j.cn112338-20200622-00872. Zhonghua Liu Xing Bing Xue Za Zhi. 2021. PMID: 34814465 Chinese.
-
The distribution and correlates of self-rated health in elderly Chinese: the China Kadoorie Biobank study.BMC Geriatr. 2019 Jun 14;19(1):168. doi: 10.1186/s12877-019-1183-2. BMC Geriatr. 2019. PMID: 31200646 Free PMC article.
Cited by
-
Trends and Challenges of Wearable Multimodal Technologies for Stroke Risk Prediction.Sensors (Basel). 2021 Jan 11;21(2):460. doi: 10.3390/s21020460. Sensors (Basel). 2021. PMID: 33440697 Free PMC article. Review.
-
Prospective Effects of Self-Rated Health on Dementia Risk in Two Twin Studies of Aging.Behav Genet. 2024 Jul;54(4):307-320. doi: 10.1007/s10519-024-10182-1. Epub 2024 Jun 1. Behav Genet. 2024. PMID: 38822218 Free PMC article.
-
Cost-Effectiveness of a Workplace-Based Hypertension Management Program in Real-World Practice in the Kailuan Study.J Am Heart Assoc. 2024 Apr 16;13(8):e031578. doi: 10.1161/JAHA.123.031578. Epub 2024 Apr 2. J Am Heart Assoc. 2024. PMID: 38563379 Free PMC article.
-
Cost-Effectiveness of Drug Treatment for Chinese Patients With Stage I Hypertension According to the 2017 Hypertension Clinical Practice Guidelines.Hypertension. 2020 Sep;76(3):750-758. doi: 10.1161/HYPERTENSIONAHA.119.14533. Epub 2020 Jul 27. Hypertension. 2020. PMID: 32713271 Free PMC article.
-
Self-rated health after stroke: a systematic review of the literature.BMC Neurol. 2019 Sep 7;19(1):221. doi: 10.1186/s12883-019-1448-6. BMC Neurol. 2019. PMID: 31493791 Free PMC article.
References
-
- Wang Z, Hu S, Sang S, Luo L, Yu C. Age-period-cohort analysis of stroke mortality in China: data from the global burden of disease study 2013. Stroke. 2017;48:271–275. - PubMed
-
- Wang W, Jiang B, Sun H, Ru X, Sun D, Wang L, et al. Prevalence, incidence, and mortality of stroke in China: results from a nationwide population-based survey of 480 687 adults. Circulation. 2017;135:759–771. - PubMed
-
- Wang J, An Z, Li B, Yang L, Tu J, Gu H, et al. Increasing stroke incidence and prevalence of risk factors in a low-income Chinese population. Neurology. 2015;84:374–381. - PubMed
-
- Guo Y, Wang H, Tian Y, Wang Y, Lip GY. Multiple risk factors and ischaemic stroke in the elderly Asian population with and without atrial fibrillation. An analysis of 425,600 Chinese individuals without prior stroke. Thromb Haemost. 2016;115:184–192. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
