

The Use of Tubular Retractors for Translaminar Discectomy for Cranially and Caudally Extruded Discs
- PMID: 29887637
- PMCID: PMC5961272
- DOI: 10.4103/ortho.IJOrtho_364_16
The Use of Tubular Retractors for Translaminar Discectomy for Cranially and Caudally Extruded Discs
Abstract
Background: The conventional interlaminar approach is adequate for access to most disc herniations in lumbar spine surgery. The access to cranially and caudally migrated disc fragments, by conventional interlaminar fenestration, requires an extension of the fenestration with the potential destruction of the facet joint complex and consequent postsurgical instability. To describe the technique and results of the translaminar technique of targeted discectomy using tubular retractors for the surgical treatment of cranially and caudally extruded discs.
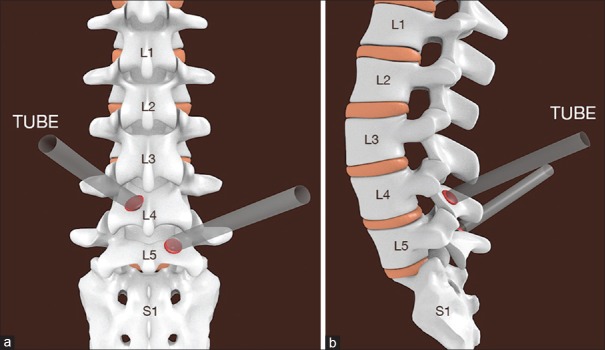
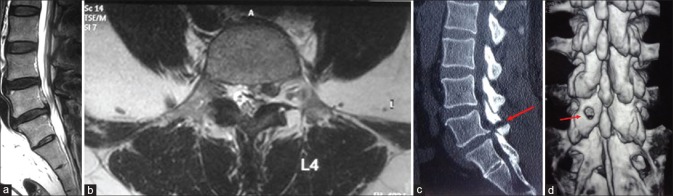
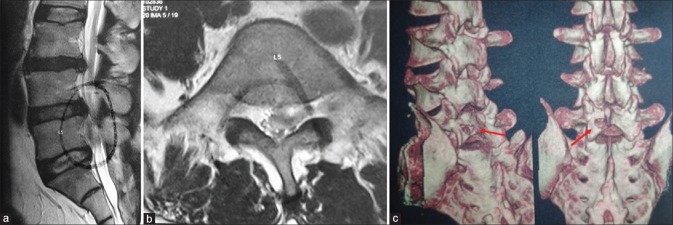
Materials and methods: The study period extended from January 2008 to December 2014. All patients with lumbar herniated discs who failed conservative management were selected for surgery and underwent routine erect radiographs and magnetic resonance imaging (MRI) of the lumbar spine. The patients with cranially or caudally migrated discs were included in this study. The technique involves approaching migrated disc through an oval window (sculpted through an 18 mm tubular retractor using a burr) in the lamina precisely over the location of the migrated disc as predicted by the preoperative MRI (inferior lamina for inferior migration and superior lamina for superior migration). The perioperative parameters studied were operative time, blood loss, complications, Oswestry Disability Index (ODI), and visual analog scale (VAS) for leg pain before surgery and at last followup. In the study, 4 patients underwent a postoperative computed tomography-scan with a three-dimensional reconstruction to visualize the oval window and to rule out any pars fracture. All technical difficulties and complications were analyzed.
Results: 17 patients in the age group of 41-58 years underwent the translaminar technique of targeted discectomy. The migration of disc was cranial in 12 patients and caudal in 5 patients. Fourteen of the affected discs were at the L4-L5 level and three were at the L5-S1 level. The mean VAS (leg pain) scale improved from 8 to 1 and the mean ODI changed from 59.8 to 23.6. There were no intraoperative or postoperative complications encountered in this study. Furthermore, no patient in the present study required a conventional laminotomy or medial facetectomy. There was no evidence of iatrogenic pars injury or instability at the last followup. There were no recurrences till the last followup.
Conclusions: The targeted translaminar approach preserves structures important for segmental spinal stability thus causing minimal anatomical disruption. This approach allows access to the extruded disc fragment and intervertebral disc space comparable to classical approaches.
Keywords: Laminotomy; Magnetic resonance imaging; intervertebral disc; lumbar vertebrae; migrated discs; minimally invasive surgery; nucleolysis; translaminar discectomy.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
The translaminar approach to canalicular and cranio-dorsolateral lumbar disc herniations.Acta Neurochir (Wien). 2002 Apr;144(4):315-20. doi: 10.1007/s007010200043. Acta Neurochir (Wien). 2002. PMID: 12021876
-
Percutaneous Endoscopic Lumbar Discectomy via Transforaminal Approach Combined with Interlaminar Approach for L4/5 and L5/S1 Two-Level Disc Herniation.Orthop Surg. 2021 May;13(3):979-988. doi: 10.1111/os.12862. Epub 2021 Apr 5. Orthop Surg. 2021. PMID: 33821557 Free PMC article.
-
The translaminar approach in combination with a tubular retractor system for the treatment of far cranio-laterally and foraminally extruded lumbar disc herniations.Zentralbl Neurochir. 2007 Feb;68(1):24-8. doi: 10.1055/s-2007-968165. Zentralbl Neurochir. 2007. PMID: 17487805
-
A Modified Approach for Minimally Invasive Tubular Microdiscectomy for Far Lateral Disc Herniations: Docking at the Caudal Level Transverse Process.Medicina (Kaunas). 2022 May 5;58(5):640. doi: 10.3390/medicina58050640. Medicina (Kaunas). 2022. PMID: 35630057 Free PMC article. Review.
-
A Simple "Involute" Technique for Successful Removal of a Caudally Migrated "Viatorr" Stent Graft.Semin Intervent Radiol. 2024 Mar 14;41(1):92-96. doi: 10.1055/s-0044-1779710. eCollection 2024 Feb. Semin Intervent Radiol. 2024. PMID: 38495265 Free PMC article. Review. No abstract available.
Cited by
-
Is Asia truly a hotspot of contemporary minimally invasive and endoscopic spinal surgery?J Spine Surg. 2020 Jan;6(Suppl 1):S224-S236. doi: 10.21037/jss.2019.12.13. J Spine Surg. 2020. PMID: 32195430 Free PMC article.
-
Trans-Tubular Translaminar Microscopic-Assisted Nucleotomy for Lumbar Disc Herniations in the Hidden Zone.Global Spine J. 2022 Sep;12(7):1420-1427. doi: 10.1177/2192568221990421. Epub 2021 Feb 3. Global Spine J. 2022. PMID: 33530710 Free PMC article.
-
Surgeon training and clinical implementation of spinal endoscopy in routine practice: results of a global survey.J Spine Surg. 2020 Jan;6(Suppl 1):S237-S248. doi: 10.21037/jss.2019.09.32. J Spine Surg. 2020. PMID: 32195431 Free PMC article.
-
Regional variations in acceptance, and utilization of minimally invasive spinal surgery techniques among spine surgeons: results of a global survey.J Spine Surg. 2020 Jan;6(Suppl 1):S260-S274. doi: 10.21037/jss.2019.09.31. J Spine Surg. 2020. PMID: 32195433 Free PMC article.
References
-
- Caspar W, Campbell B, Barbier DD, Kretschmmer R, Gotfried Y. The Caspar microsurgical discectomy and comparison with a conventional standard lumbar disc procedure. Neurosurgery. 1991;28:78–86. - PubMed
-
- Epstein NE. Evaluation of varied surgical approaches used in the management of 170 far-lateral lumbar disc herniations: Indications and results. J Neurosurg. 1995;83:648–56. - PubMed
-
- Garrido E, Connaughton PN. Unilateral facetectomy approach for lateral lumbar disc herniation. J Neurosurg. 1991;74:754–6. - PubMed
-
- Kunogi J, Hasue M. Diagnosis and operative treatment of intraforaminal and extraforaminal nerve root compression. Spine (Phila Pa 1976) 1991;16:1312–20. - PubMed
-
- Di Lorenzo N, Porta F, Onnis G, Cannas A, Arbau G, Maleci A. Pars interarticularis fenestration in the treatment of foraminal lumbar disc herniation: A further surgical approach. Neurosurgery. 1998;42:87–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous