

Efficacy and safety of dapagliflozin in patients with type 2 diabetes and moderate renal impairment (chronic kidney disease stage 3A): The DERIVE Study
- PMID: 29888547
- PMCID: PMC6175614
- DOI: 10.1111/dom.13413
Efficacy and safety of dapagliflozin in patients with type 2 diabetes and moderate renal impairment (chronic kidney disease stage 3A): The DERIVE Study
Erratum in
-
CORRIGENDUM.Diabetes Obes Metab. 2019 Jan;21(1):203. doi: 10.1111/dom.13563. Epub 2018 Nov 8. Diabetes Obes Metab. 2019. PMID: 30516008 Free PMC article. No abstract available.
Abstract
Aims: Dapagliflozin is a selective inhibitor of sodium glucose co-transporter 2 (SGLT2). This study assessed the efficacy and safety of dapagliflozin 10 mg vs placebo in patients with type 2 diabetes (T2D) and moderate renal impairment (estimated glomerular filtration rate [eGFR], 45-59 mL/min/1.73 m2 ; chronic kidney disease [CKD] stage 3A).
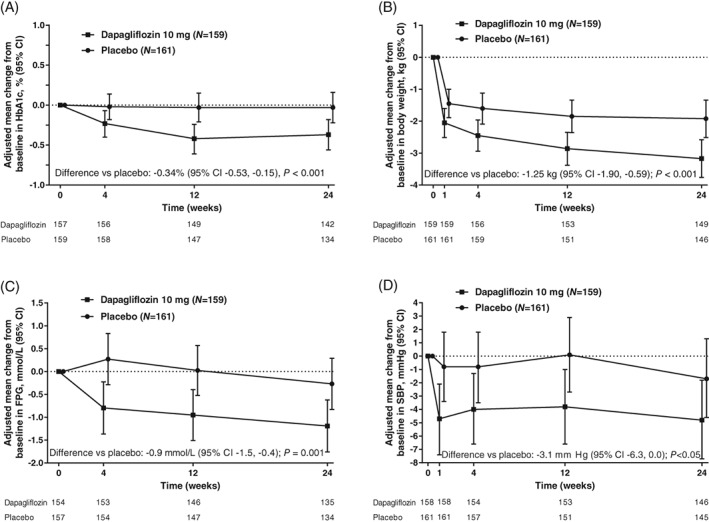
Materials and methods: In this double-blind, parallel group, Phase 3 study (NCT02413398, clinicaltrials.gov) patients with inadequately controlled T2D (HbA1c 7.0%-11.0%) were randomized (1:1) to dapagliflozin 10 mg once daily (N = 160) or matching placebo (N = 161) for 24 weeks. Randomization was stratified by pre-enrolment glucose-lowering therapy. The primary endpoint was change from baseline in HbA1c at Week 24.
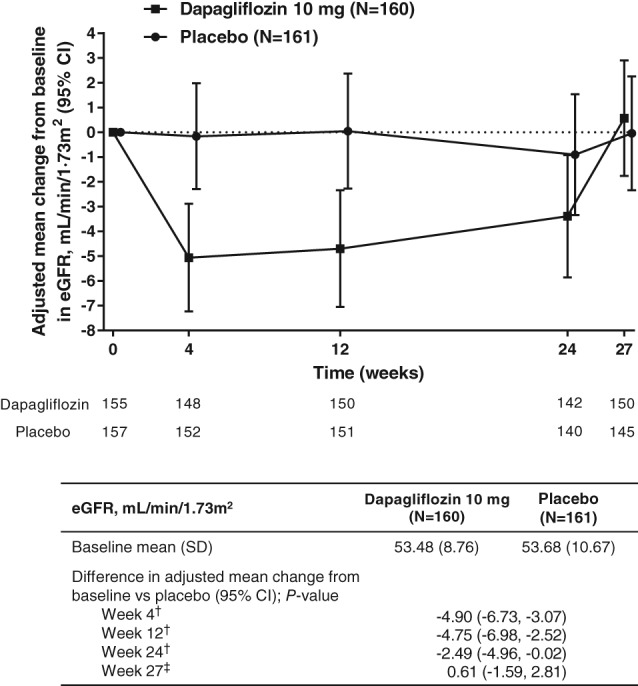
Results: At Week 24, compared with placebo, dapagliflozin significantly decreased HbA1c (difference [95% CI], -0.34% [-0.53, -0.15]; P < 0.001), body weight (difference [95% CI], -1.25 kg [-1.90, -0.59]; P < 0.001), fasting plasma glucose (difference [95% CI], -0.9 mmol/L [-1.5, -0.4]; P = 0.001) and systolic blood pressure (difference [95% CI], -3.1 mm Hg [-6.3, 0.0]; P < 0.05). Decreases from baseline in eGFR were greater with dapagliflozin than placebo at Week 24 (-2.49 mL/min/1.73 m2 [-4.96, -0.02]), however, eGFR returned to baseline levels at Week 27 (3 weeks post-treatment) (0.61 mL/min/1.73 m2 [-1.59, 2.81]). No increase in adverse events (AEs; 41.9% vs 47.8%) or serious AEs (5.6% vs 8.7%) were reported with dapagliflozin versus placebo. No AEs of bone fractures, amputations or DKA were reported.
Conclusions: The findings of this study (NCT02413398, clinicaltrials.gov) support the positive benefit/risk profile of dapagliflozin for the treatment of patients with T2D and CKD 3A.
© 2018 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
P. F. has served as an advisory board member and speaker for AstraZeneca, Eli Lilly and Boehringer Ingelheim. S. D. P. has served on advisory boards for AstraZeneca, Boehringer Ingelheim, Eli Lilly, GlaxoSmithKline, Intarcia, Janssen, Merck, Novartis, Novo Nordisk A/S, Laboratoires Servier, Sanofi and Takeda; has been a research investigator for Merck, Novartis and Takeda; and has been a speaker for Boehringer Ingelheim, Novartis and Takeda. J. B. B. has received contracted consulting fees, paid to his institution, and travel support from Adocia, AstraZeneca, Dexcom, Elcelyx Therapeutics, Eli Lilly, Intarcia Therapeutics, Lexicon, Metavention, NovaTarg, Novo Nordisk, Sanofi, and vTv Therapeutics; has received grant support from AstraZeneca, Boehringer Ingelheim, Johnson & Johnson, Lexicon, Novo Nordisk, Sanofi, Theracos and vTv Therapeutics; has served on the board of the AstraZeneca HealthCare Foundation; and holds stock options in Mellitus Health and PhaseBio. R. G. has served on advisory boards for Amgen, Abbott, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck, Novo Nordisk, Sanofi, Takeda and Valeant; has served as a research investigator for AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck, Novo Nordisk, Sanofi and Takeda; and has been a speaker for Amgen, Abbott, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck, Mylan, Novo Nordisk, Sanofi, Laboratoires Servier and Valeant. F. G. has served as an advisory board member for AstraZeneca; has served as a research investigator for Eli Lilly; has served as a speaker for AstraZeneca and Eli Lilly; has received consulting fees from AstraZeneca, Sanofi, Abbott, Boehringer Ingelheim, Eli Lilly, MedImmune, Merck Sharp & Dohme and Roche Diabetes Care; and has received grants from Lifescan, Eli Lilly and Takeda. D. R. is an employee of AstraZeneca. A. M. L., C. D. S. and P. S. are employees of and shareholders in AstraZeneca.
Figures
References
-
- Kramer H, Molitch ME. Screening for kidney disease in adults with diabetes. Diabetes Care. 2005;28:1813‐1816. - PubMed
-
- Foundation NK . Diabetes and chronic kidney disease. 2016. https://www.kidney.org/news/newsroom/factsheets/Diabetes-And-CKD. Accessed March 13, 2018.
-
- KDOQI clinical practice guideline for diabetes and CKD: 2012 update. Am J Kidney Dis. 2012;60:850‐886. - PubMed
-
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes, 2015: a patient‐centred approach. Update to a position statement of the American Diabetes Association and the European Association for the Study of diabetes. Diabetologia. 2015;58:429‐442. - PubMed
-
- Cavanaugh KL. Diabetes management issues for patients with chronic kidney disease. Clin Diabetes. 2007;25:90‐97.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
