

Comparison of the Cumulative Efficacy and Safety of Chloroquine, Artesunate, and Chloroquine-Primaquine in Plasmodium vivax Malaria
- PMID: 29889239
- PMCID: PMC6206118
- DOI: 10.1093/cid/ciy319
Comparison of the Cumulative Efficacy and Safety of Chloroquine, Artesunate, and Chloroquine-Primaquine in Plasmodium vivax Malaria
Abstract
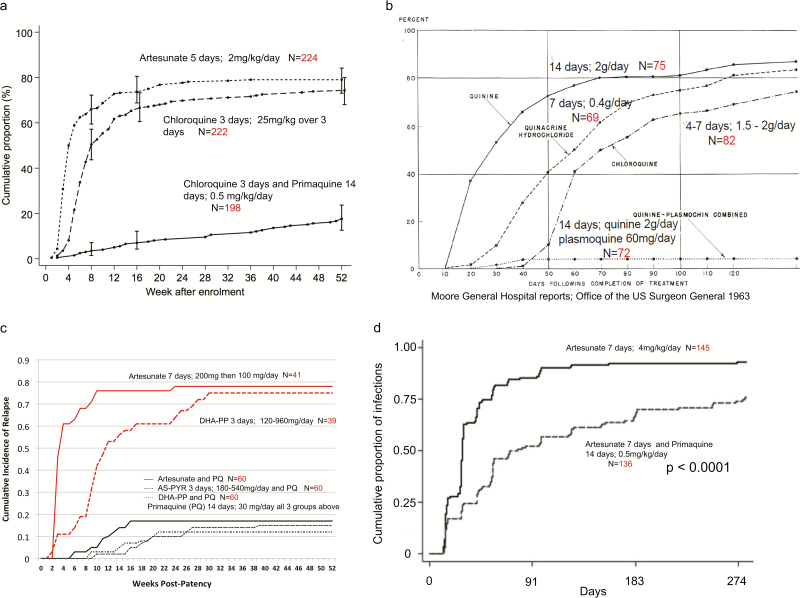
Background: Chloroquine has been recommended for Plasmodium vivax infections for >60 years, but resistance is increasing. To guide future therapies, the cumulative benefits of using slowly eliminated (chloroquine) vs rapidly eliminated (artesunate) antimalarials, and the risks and benefits of adding radical cure (primaquine) were assessed in a 3-way randomized comparison conducted on the Thailand-Myanmar border.
Methods: Patients with uncomplicated P. vivax malaria were given artesunate (2 mg/kg/day for 5 days), chloroquine (25 mg base/kg over 3 days), or chloroquine-primaquine (0.5 mg/kg/day for 14 days) and were followed for 1 year. Recurrence rates and their effects on anemia were compared.
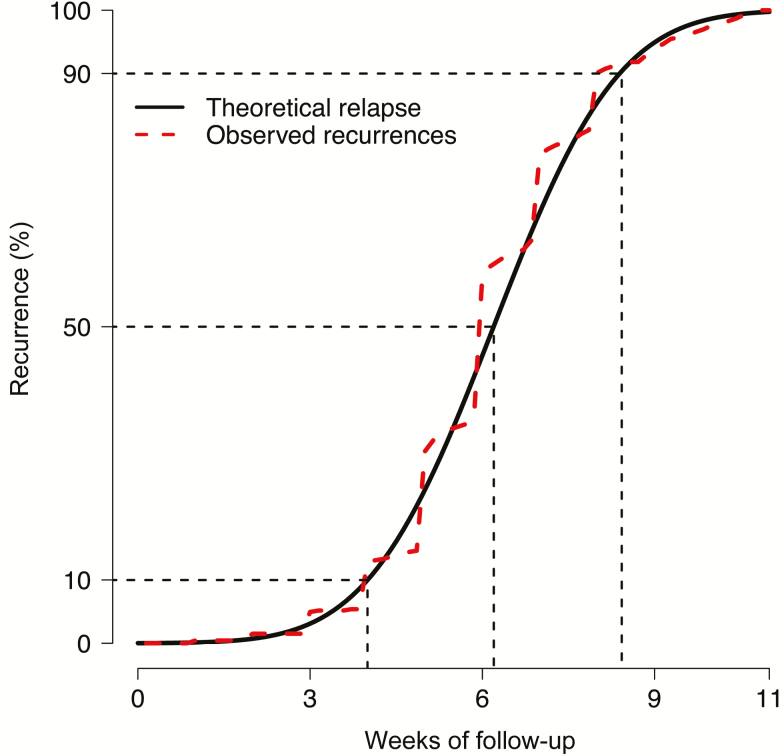
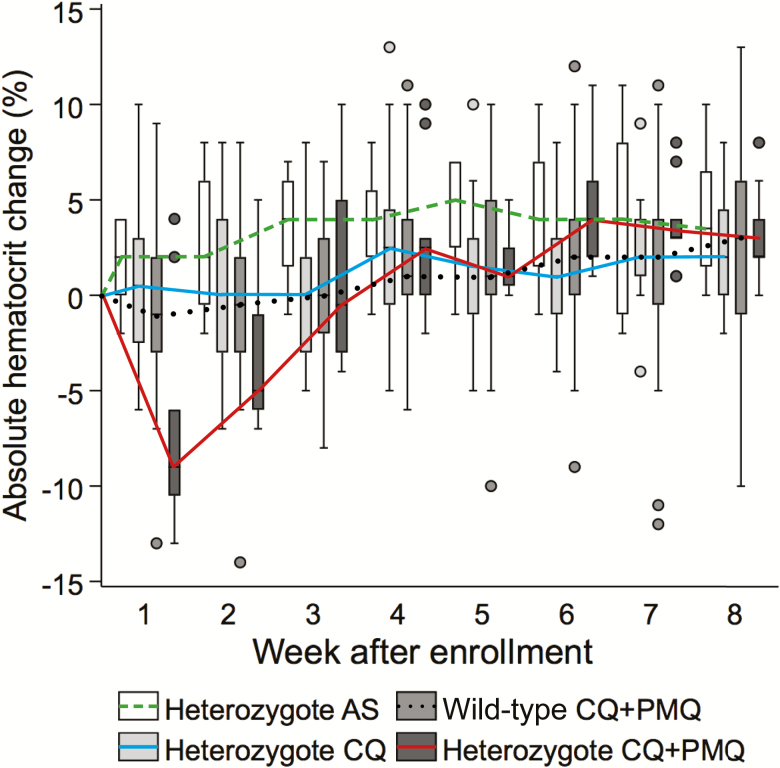
Results: Between May 2010 and October 2012, 644 patients were enrolled. Artesunate cleared parasitemia significantly faster than chloroquine. Day 28 recurrence rates were 50% with artesunate (112/224), 8% with chloroquine (18/222; P < .001), and 0.5% with chloroquine-primaquine (1/198; P < .001). Median times to first recurrence were 28 days (interquartile range [IQR], 21-42) with artesunate, 49 days (IQR, 35-74) with chloroquine, and 195 days (IQR, 82-281) with chloroquine-primaquine. Recurrence by day 28, was associated with a mean absolute reduction in hematocrit of 1% (95% confidence interval [CI], .3%-2.0%; P = .009). Primaquine radical cure reduced the total recurrences by 92.4%. One-year recurrence rates were 4.51 (95% CI, 4.19-4.85) per person-year with artesunate, 3.45 (95% CI, 3.18-3.75) with chloroquine (P = .002), and 0.26 (95% CI, .19-.36) with chloroquine-primaquine (P < .001).
Conclusions: Vivax malaria relapses are predominantly delayed by chloroquine but prevented by primaquine.
Clinical trials registration: NCT01074905.
Figures
References
-
- Whorton CM, Kirschbaum WR. The Chesson strain of Plasmodium vivax malaria; factors influencing the incubation period. J Infect Dis 1947; 80:223–7. - PubMed
-
- Baird JK, Leksana B, Masbar S et al. . Diagnosis of resistance to chloroquine by Plasmodium vivax: timing of recurrence and whole blood chloroquine levels. Am J Trop Med Hyg 1997; 56:621–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
