

Hybrid Therapy for Metastatic Epidural Spinal Cord Compression: Technique for Separation Surgery and Spine Radiosurgery
- PMID: 29889256
- PMCID: PMC7189205
- DOI: 10.1093/ons/opy137
Hybrid Therapy for Metastatic Epidural Spinal Cord Compression: Technique for Separation Surgery and Spine Radiosurgery
Erratum in
-
Hybrid Therapy for Metastatic Epidural Spinal Cord Compression: Technique for Separation Surgery and Spine Radiosurgery.Oper Neurosurg. 2018 Sep 1;15(3):361. doi: 10.1093/ons/opy203. Oper Neurosurg. 2018. PMID: 30053186 Free PMC article. No abstract available.
Abstract
Background: Despite major advances in radiation and systemic treatments, surgery remains a critical step in the multidisciplinary treatment of metastatic spinal cord tumors.
Objective: To describe the indications, rationale, and technique of "hybrid therapy" (separation surgery and concomitant spine stereotactic radiosurgery [SRS]) along with practical nuances.
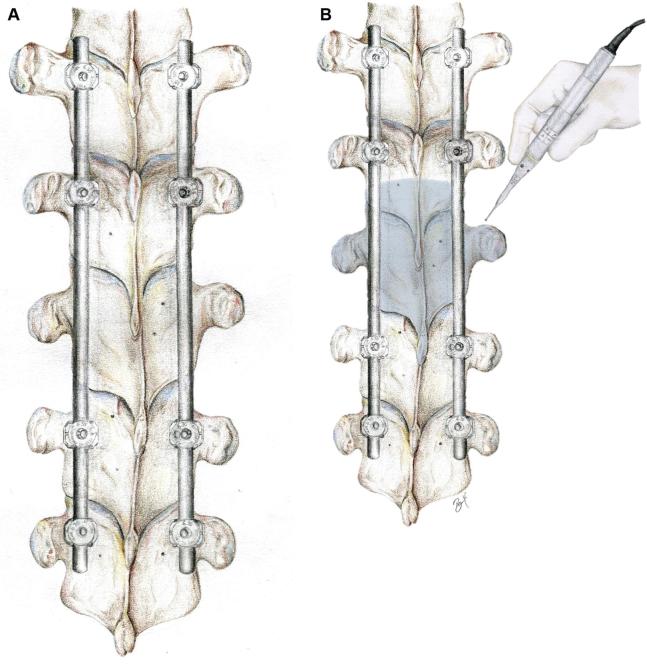
Methods: Separation surgery describes a posterolateral approach for circumferential epidural decompression and stabilization. The goal is to decompress the spinal cord, stabilize the spine, and create adequate separation between the neural elements and the tumor for SRS to achieve durable tumor control.
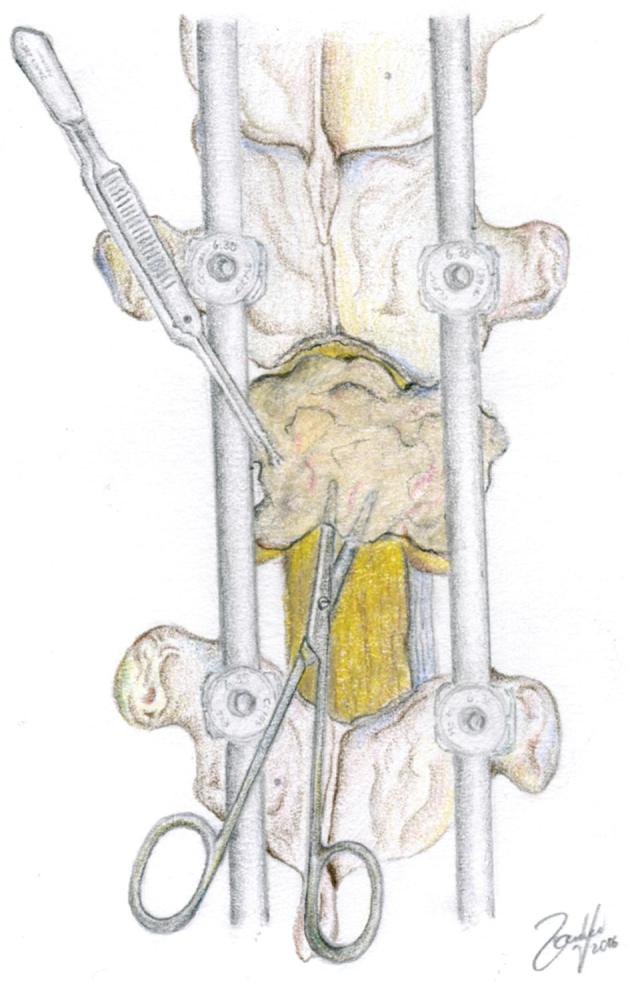
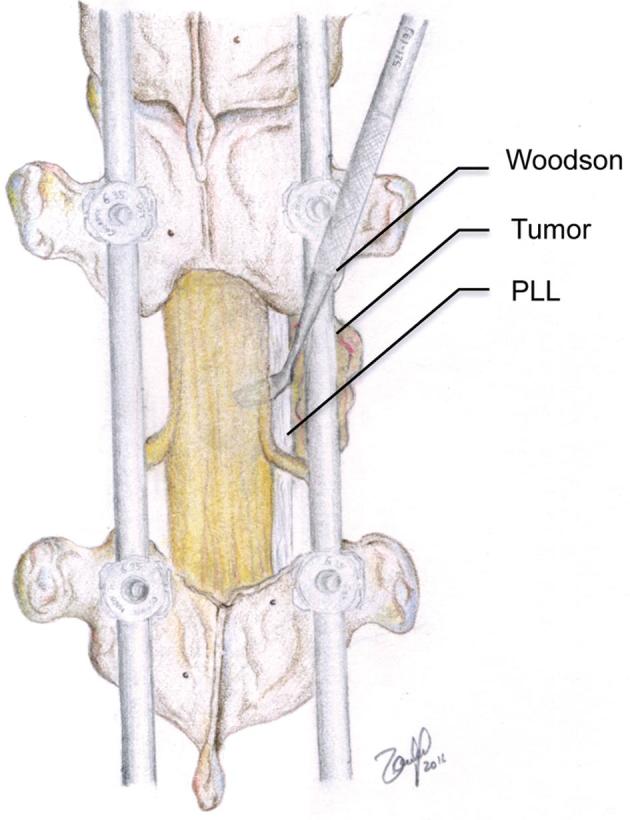
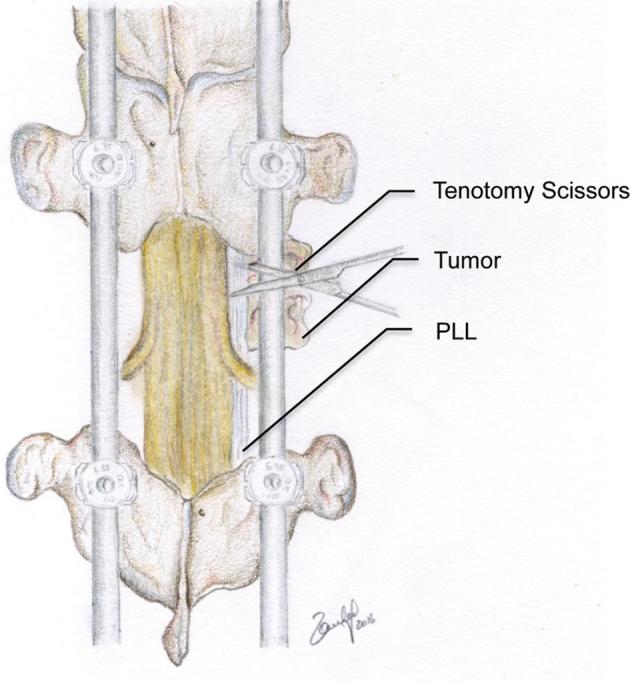
Results: A transpedicular route to achieve ventrolateral access and limited resection of the tumorous vertebral body is carried out. In the setting of high-grade cord compression, caution must be taken when performing the tumor decompression. "Separation" of the ventral epidural tumor component anteriorly creates space for concomitant SRS while a simple laminectomy would not adequately achieve this goal. Dissection of the posterior longitudinal ligament allows maximal ventral decompression. Gross total tumor resection is not crucial for durable tumor control using the "hybrid therapy" model. Thus, attempts at ventral tumor resection may unnecessarily increase operative morbidity. Cement augmentation of the construct or vertebral body may improve construct stability. CT myelogram is the preferred exam for postoperative SRS planning. Radiosurgical planning constitutes a multidisciplinary effort and guidelines for contouring in the postoperative setting have recently become available.
Conclusion: Separation surgery is an effective, well-tolerated, and reproducible surgery. It provides safe margins for concomitant SRS. Combined, this "Hybrid Therapy" allows durable local control, maintenance of spinal stability, and palliation of symptoms, while minimizing operative morbidity.
Keywords: Hybrid therapy; Radiosurgery; Separation Surgery; Tumor.
Copyright © 2018 by the Congress of Neurological Surgeons.
Figures
References
-
- Klimo P Jr, Kestle JR, Schmidt MH. Clinical trials and evidence-based medicine for metastatic spine disease. Neurosurg Clin N Am. 2004;15(4):549-564. - PubMed
-
- Ortiz Gomez JA. The incidence of vertebral body metastases. Int Orthop. 1995;19(5):309-311. - PubMed
-
- Bilsky M, Smith M. Surgical approach to epidural spinal cord compression. Hematol Oncol Clin North Am.. 2006;20(6):1307-1317. - PubMed
-
- Patchell RA, Tibbs PA, Regine WFet al.. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: A randomised trial. Lancet North Am Ed. 2005;366(9486):643-648. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
