

Non-recovery from dialysis-requiring acute kidney injury and short-term mortality and cardiovascular risk: a cohort study
- PMID: 29890946
- PMCID: PMC5996504
- DOI: 10.1186/s12882-018-0924-3
Non-recovery from dialysis-requiring acute kidney injury and short-term mortality and cardiovascular risk: a cohort study
Abstract
Background: The high mortality and cardiovascular disease (CVD) burden in patients with end-stage renal disease (ESRD) is well-documented. Recent literature suggests that acute kidney injury is also associated with CVD. It is unknown whether patients with incident ESRD due to dialysis-requiring acute kidney injury (AKI-D) are at higher short-term risk for death and CVD events, compared with incident ESRD patients without preceding AKI-D. Few studies have examined the impact of recovery from AKI-D on subsequent CVD risk.
Methods: In this retrospective cohort study, we evaluated adult members of Kaiser Permanente Northern California who initiated dialysis from January 2009 to September 2015. Preceding AKI-D and subsequent outcomes of death and CVD events (acute coronary syndrome, heart failure, ischemic stroke or transient ischemic attack) were identified from electronic health records. We performed multivariable Cox regression models adjusting for demographics, comorbidities, medication use, and laboratory results.
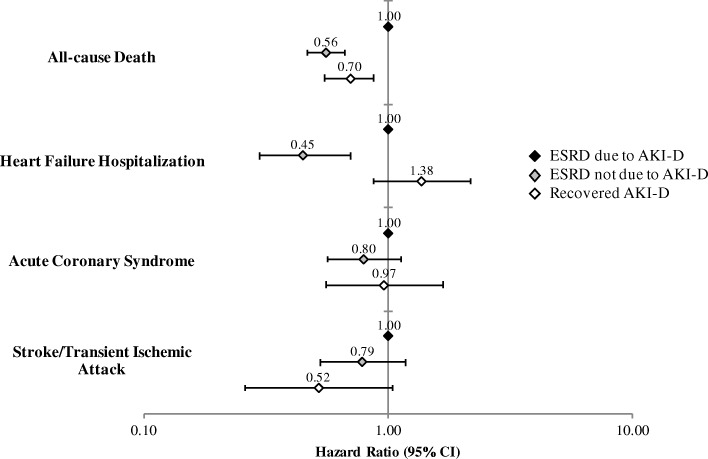
Results: Compared to incident ESRD patients who experienced AKI-D (n = 1865), patients with ESRD not due to AKI-D (n = 3772) had significantly lower adjusted rates of death (adjusted hazard ratio [aHR] 0.56, 95% CI: 0.47-0.67) and heart failure hospitalization (aHR 0.45, 0.30-0.70). Compared to AKI-D patients who did not recover and progressed to ESRD, AKI-D patients who recovered (n = 1347) had a 30% lower adjusted relative rate of death (aHR 0.70, 0.55-0.88).
Conclusions: Patients who transition to ESRD via AKI-D are a high-risk subgroup that may benefit from aggressive monitoring and medical management, particularly for heart failure. Recovery from AKI-D is independently associated with lower short-term mortality.
Keywords: Cardiovascular events; Dialysis-requiring acute kidney injury; End-stage renal disease; Mortality; Renal recovery.
Conflict of interest statement
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki and was approved by the KPNC and University of California, San Francisco institutional review boards. We obtained a waiver of informed consent given the nature of the study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Bradbury BD, Fissell RB, Albert JM, Anthony MS, Critchlow CW, Pisoni RL, Port FK, Gillespie BW. Predictors of early mortality among incident US hemodialysis patients in the Dialysis outcomes and practice patterns study (DOPPS) Clinical journal of the American Society of Nephrology : CJASN. 2007;2(1):89–99. doi: 10.2215/CJN.01170905. - DOI - PubMed
-
- Eckardt KU, Gillespie IA, Kronenberg F, Richards S, Stenvinkel P, Anker SD, Wheeler DC, de Francisco AL, Marcelli D, Froissart M, et al. High cardiovascular event rates occur within the first weeks of starting hemodialysis. Kidney Int. 2015;88(5):1117–1125. doi: 10.1038/ki.2015.117. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
