

Virtual Bronchoscopy-Guided Treatment Planning to Map and Mitigate Radiation-Induced Airway Injury in Lung SAbR
- PMID: 29891202
- PMCID: PMC6089651
- DOI: 10.1016/j.ijrobp.2018.04.060
Virtual Bronchoscopy-Guided Treatment Planning to Map and Mitigate Radiation-Induced Airway Injury in Lung SAbR
Abstract
Purpose: Radiation injury to the bronchial tree is an important yet poorly understood potential side effect in lung stereotactic ablative radiation therapy (SAbR). We investigate the integration of virtual bronchoscopy in radiation therapy planning to quantify dosage to individual airways. We develop a risk model of airway collapse and develop treatment plans that reduce the risk of radiation-induced airway injury.
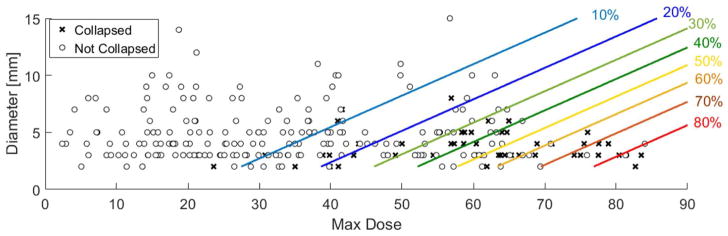
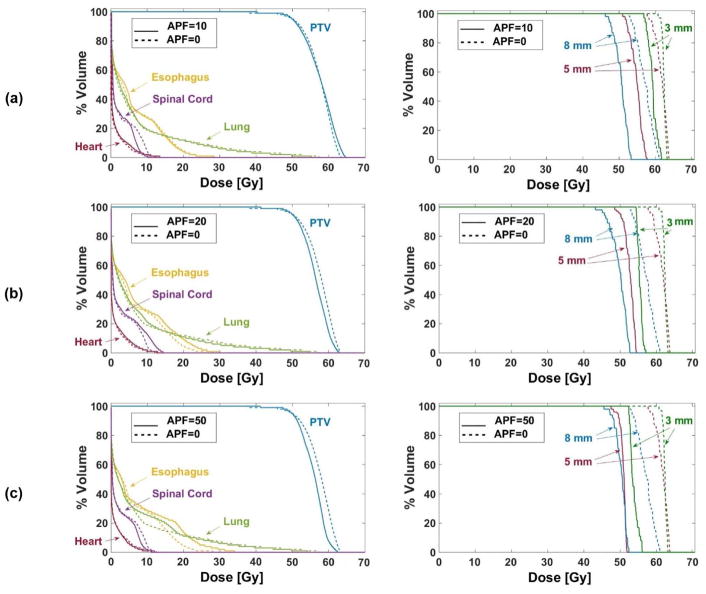
Methods and materials: Pre- and post-SAbR diagnostic-quality computerized tomography (CT) scans were retrospectively collected from 26 lung cancer patients. From each scan, the bronchial tree was segmented using a virtual bronchoscopy system and registered deformably to the planning CT. Univariate and stepwise multivariate Cox regressions were performed, examining factors such as age, comorbidities, smoking pack years, airway diameter, and maximum point dosage (Dmax). Logistic regression was utilized to formulate a risk function of segmental collapse based on Dmax and diameter. The risk function was incorporated into the objective function along with clinical dosage volume constraints for planning target volume (PTV) and organs at risk (OARs).
Results: Univariate analysis showed that segmental diameter (P = .014) and Dmax (P = .007) were significantly correlated with airway segment collapse. Multivariate stepwise Cox regression showed that diameter (P = .015), Dmax (P < .0001), and pack/years of smoking (P = .02) were significant independent factors associated with collapse. Risk management-based plans enabled significant dosage reduction to individual airway segments while fulfilling clinical dosimetric objectives.
Conclusion: To our knowledge, this is the first systematic investigation of functional avoidance in lung SAbR based on mapping and minimizing doses to individual bronchial segments. Our early results show that it is possible to substantially lower airway dosage. Such dosage reduction may potentially reduce the risk of radiation-induced airway injury, while satisfying clinically prescribed dosimetric objectives.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures



References
-
- Timmerman RD, et al. Long-term Results of RTOG 0236: A Phase II Trial of Stereotactic Body Radiation Therapy (SBRT) in the Treatment of Patients with Medically Inoperable Stage I Non-Small Cell Lung Cancer. International Journal of Radiation Oncology • Biology • Physics. 2014;90(1):S30.
-
- Chi A, et al. Systemic review of the patterns of failure following stereotactic body radiation therapy in early-stage non-small-cell lung cancer: clinical implications. Radiother Oncol. 2010;94(1):1–11. - PubMed
-
- Timmerman R, et al. Excessive toxicity when treating central tumors in a phase II study of stereotactic body radiation therapy for medically inoperable early-stage lung cancer. J Clin Oncol. 2006;24(30):4833–9. - PubMed
-
- Matsuo Y, et al. Dose--volume metrics associated with radiation pneumonitis after stereotactic body radiation therapy for lung cancer. Int J Radiat Oncol Biol Phys. 2012;83(4):e545–9. - PubMed
-
- Wisnivesky JP, et al. Radiation therapy for the treatment of unresected stage I–II non-small cell lung cancer. Chest. 2005;128(3):1461–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
