

A single-center experience of 1500 lung transplant patients
- PMID: 29891245
- PMCID: PMC6939473
- DOI: 10.1016/j.jtcvs.2018.03.112
A single-center experience of 1500 lung transplant patients
Abstract
Objective: Over the past 30 years, lung transplantation has emerged as the definitive treatment for end-stage lung disease. In 2005, the lung allocation score (LAS) was introduced to allocate organs according to disease severity. The number of transplants performed annually in the United States continues to increase as centers have become more comfortable expanding donor and recipient criteria and have become more facile with the perioperative and long-term management of these patients. We report a single-center experience with lung transplants, looking at patients before and after the introduction of LAS.
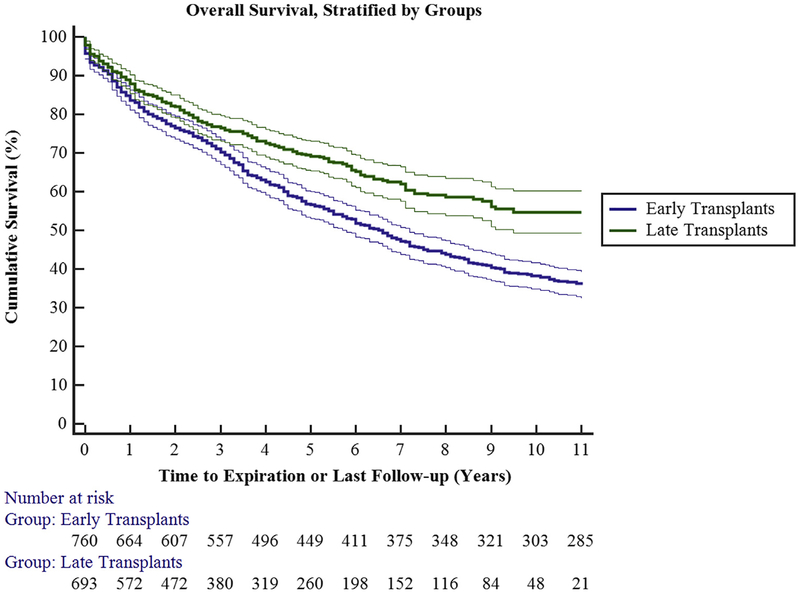
Methods: We retrospectively reviewed 1500 adult lung transplants at a single center performed between 1988 and 2016. Patients were separated into 2 groups, before and after the introduction of LAS: group 1 (April 1988 to April 2005; 792 patients) and group 2 (May 2005 to September 2016; 708 patients).
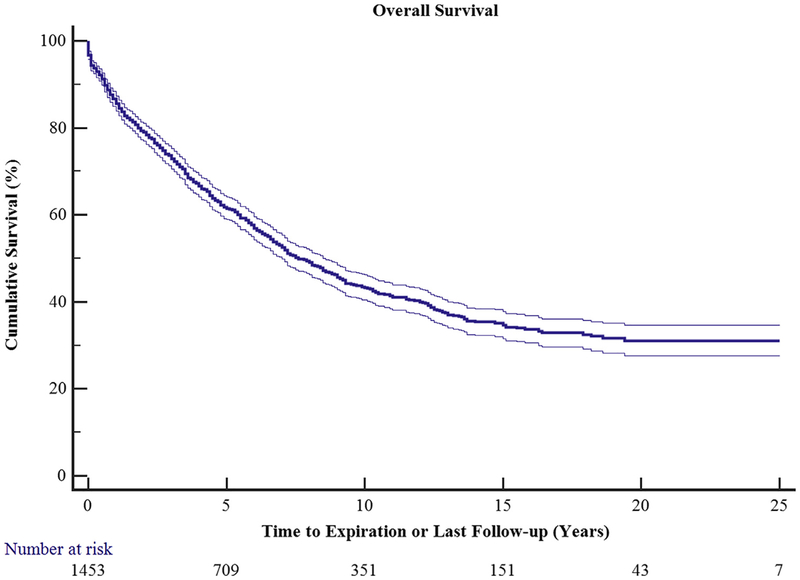
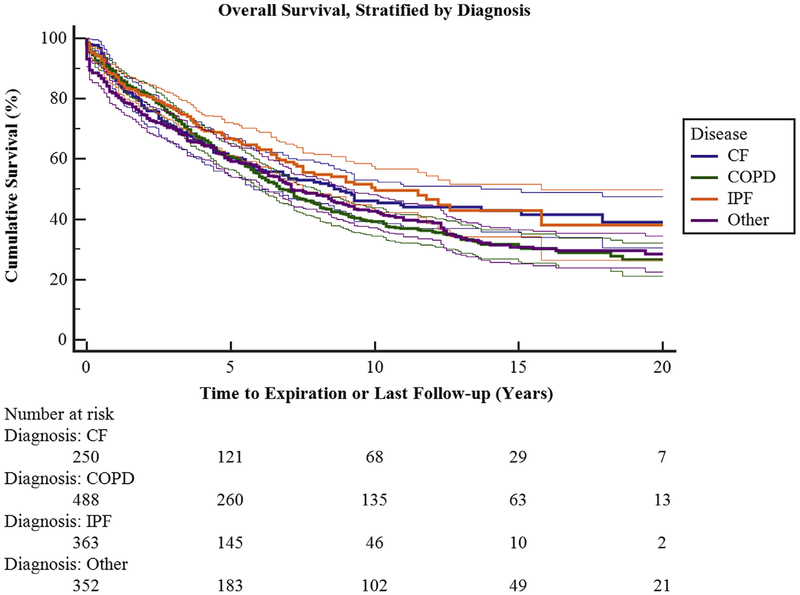
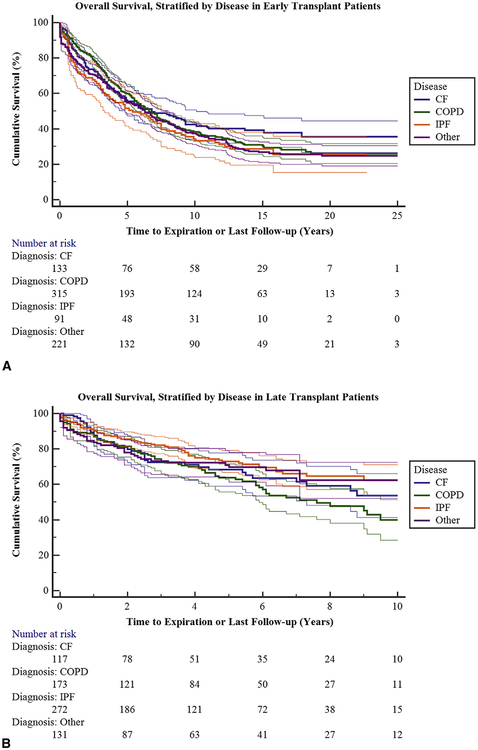
Results: Differences in demographic data were noted over these periods, reflecting changes in allocation of organs. Group 1 patient average age was 48 ± 13 years, and 404 subjects (51%) were male. Disease processes included emphysema (52%; 412), cystic fibrosis (18.2%; 144), pulmonary fibrosis (16.1%; 128) and pulmonary vascular disease (7.2%; 57). Double lung transplant (77.7%; 615) was performed more frequently than single lung transplant (22.3%; 177). Group 2 average age was 50 ± 14 years, and 430 subjects (59%) were male. Disease processes included pulmonary fibrosis (46%; 335), emphysema (25.8%; 188), cystic fibrosis (17.7%; 127) and pulmonary vascular disease (1.6%; 11). Double lung transplant (96.2%; 681) was performed more frequently than single lung transplant (3.8%; 27). Overall incidence of grade 3 primary graft dysfunction (PGD) in group 1 was significantly lower at 22.1% (175) than in group 2 at 31.6% (230) (P < .001). Nonetheless, overall hospital mortality was not statistically different between the 2 groups (4.4% vs 3.5%; P < .4). Most notably, survival at 1 year was statistically different at 646 (81.6%) for group 1 and 665 (91.4%) for group 2 (P < .02).
Conclusions: Patient demographics over the study period have changed with an increased number of fibrotic patients transplanted. In addition, more aggressive strategies with donor/recipient selection appear to have resulted in a higher incidence of primary graft dysfunction. This does not, however, appear to affect patient survival on index hospitalization or at 1 year. In fact, we have observed a significant improvement in survival at 1 year in the more recent era. This observation suggests that continued expansion of possible donors and recipients, coupled with a more sophisticated understanding of primary graft dysfunction and long-term chronic rejection, can lead to increased transplant volume and prolonged survival.
Keywords: bronchiolitis obliterans; chronic rejection; cystic fibrosis; emphysema; lung allocation score; lung transplantation; primary graft dysfunction; pulmonary fibrosis.
Copyright © 2018 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Statement
Authors have nothing to disclose with regard to commercial support.
Figures
Comment in
-
Living by numbers.J Thorac Cardiovasc Surg. 2018 Aug;156(2):906-907. doi: 10.1016/j.jtcvs.2018.04.002. Epub 2018 Apr 12. J Thorac Cardiovasc Surg. 2018. PMID: 29754792 No abstract available.
-
Lung transplantation and beyond: continued challenges in the wake of significant progress.J Thorac Dis. 2019 Mar;11(Suppl 3):S413-S416. doi: 10.21037/jtd.2018.11.112. J Thorac Dis. 2019. PMID: 30997234 Free PMC article. No abstract available.
References
-
- Yusen RD, Edwards LB, Dipchand AI, Goldfarb SB, Kucheryavaya AY, Levvy BJ, et al. The registry of the International Society for Heart and Lung Transplantation: thirty-third adult lung and heart-lung transplant report–2016; Focus theme: primary diagnostic indications for transplant. J Heart Lung Transplant. 2016;35:1170–84. - PubMed
-
- Meyers BF, de la Morena M, Sweet SC, Trulock EP, Guthrie TJ, Mendeloff EN, et al. Primary graft dysfunction and other selected complications of lung transplantation: a single-center experience of 983 patients. J Thorac Cardiovasc Surg. 2005;129:1421–9. - PubMed
-
- Kreisel D, Krupnick AS, Puri V, Guthrie TJ, Trulock EP, Meyers BF, Patterson GA. Short- and long-term outcomes of 1000 adult lung transplant recipients at a single center. J Thorac Cardiovasc Surg. 2011;141:215–22. - PubMed
-
- Snell GI, Yusen RD, Weill D, Strueber M, Garrity E, Reed A, et al. Report of the ISHLT working group on primary lung graft dysfunction, part I: definition and grading-A 2016 consensus group statement of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 2017;36:1097–103. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
