

Exploratory Study of rTMS Neuromodulation Effects on Electrocortical Functional Measures of Performance in an Oddball Test and Behavioral Symptoms in Autism
- PMID: 29892214
- PMCID: PMC5985329
- DOI: 10.3389/fnsys.2018.00020
Exploratory Study of rTMS Neuromodulation Effects on Electrocortical Functional Measures of Performance in an Oddball Test and Behavioral Symptoms in Autism
Abstract
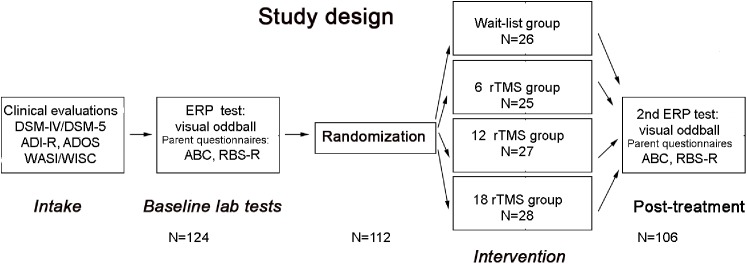
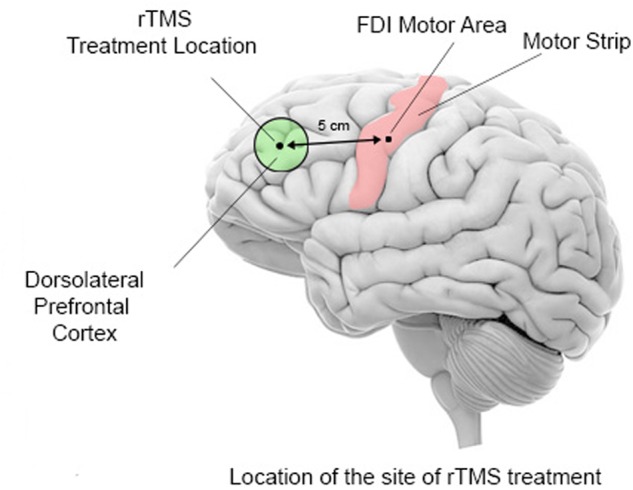
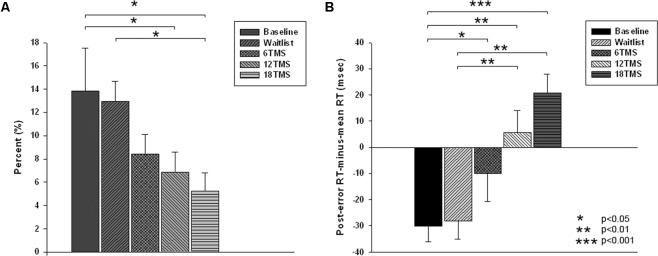
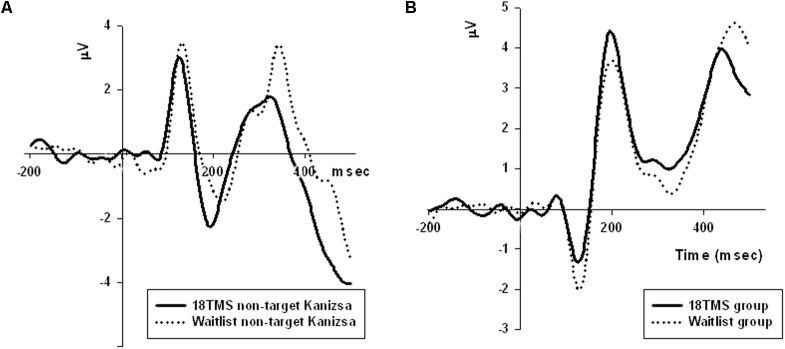
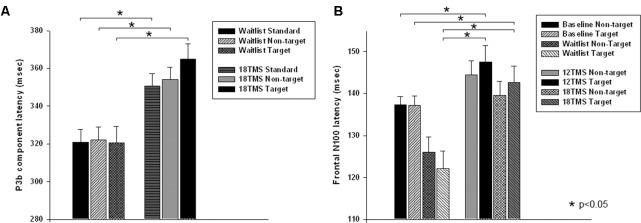
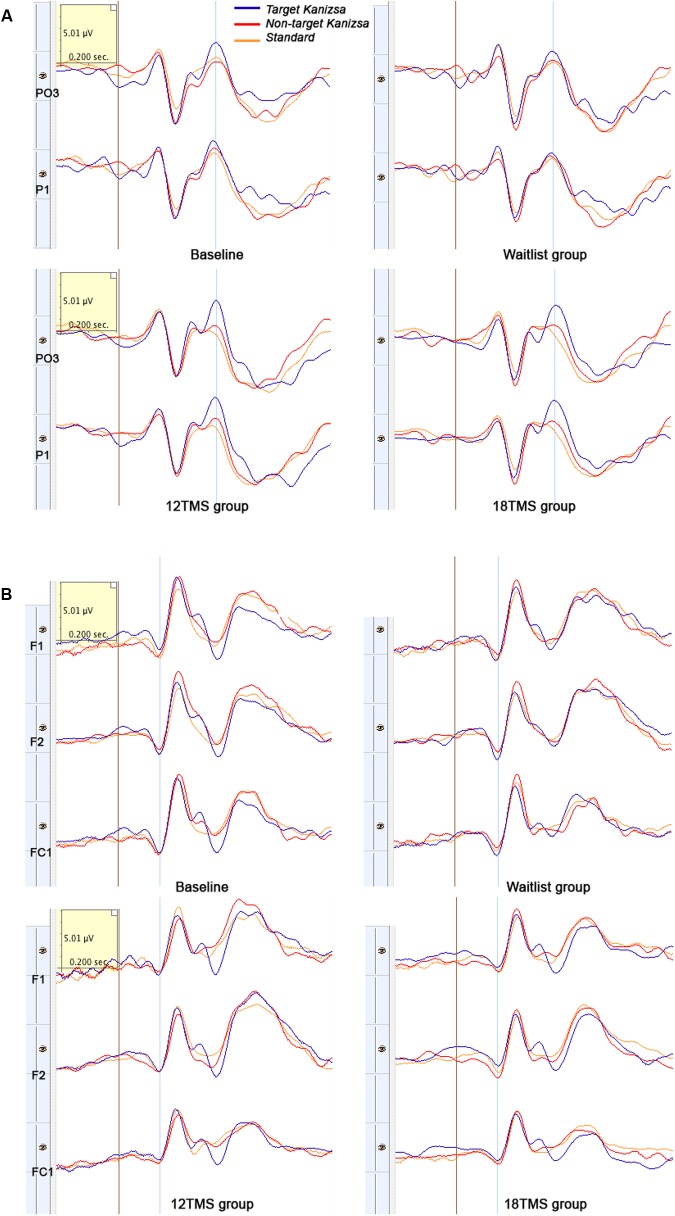
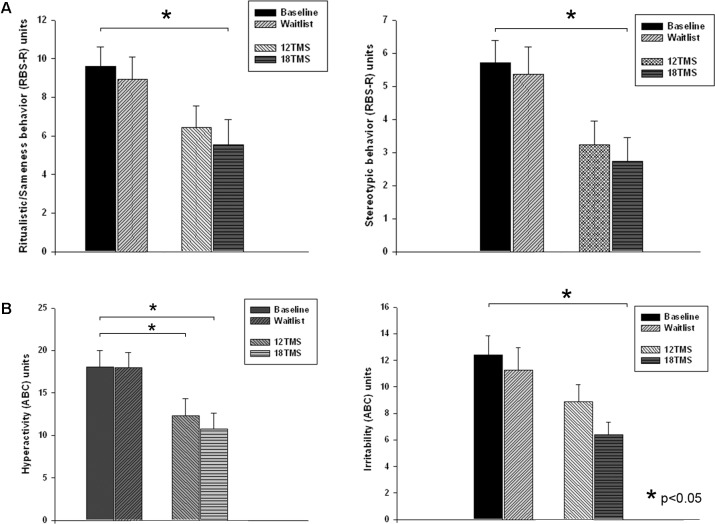
There is no accepted pathology to autism spectrum disorders (ASD) but research suggests the presence of an altered excitatory/inhibitory (E/I) bias in the cerebral cortex. Repetitive transcranial magnetic stimulation (rTMS) offers a non-invasive means of modulating the E/I cortical bias with little in terms of side effects. In this study, 124 high functioning ASD children (IQ > 80, <18 years of age) were recruited and assigned using randomization to either a waitlist group or one of three different number of weekly rTMS sessions (i.e., 6, 12, and 18). TMS consisted of trains of 1.0 Hz frequency pulses applied over the dorsolateral prefrontal cortex (DLPFC). The experimental task was a visual oddball with illusory Kanizsa figures. Behavioral response variables included reaction time and error rate along with such neurophysiological indices such as stimulus and response-locked event-related potentials (ERP). One hundred and twelve patients completed the assigned number of TMS sessions. Results showed significant changes from baseline to posttest period in the following measures: motor responses accuracy [lower percentage of committed errors, slower latency of commission errors and restored normative post-error reaction time slowing in both early and later-stage ERP indices, enhanced magnitude of error-related negativity (ERN), improved error monitoring and post-error correction functions]. In addition, screening surveys showed significant reductions in aberrant behavior ratings and in both repetitive and stereotypic behaviors. These differences increased with the total number of treatment sessions. Our results suggest that rTMS, particularly after 18 sessions, facilitates cognitive control, attention and target stimuli recognition by improving discrimination between task-relevant and task-irrelevant illusory figures in an oddball test. The noted improvement in executive functions of behavioral performance monitoring further suggests that TMS has the potential to target core features of ASD.
Keywords: ERP; TMS; aberrant and repetitive behaviors; autism spectrum disorder; executive functions; oddball task; reaction time.
Figures
References
-
- Aman M. G., Singh N. N. (1994). Aberrant Behavior Checklist—Community. Supplementary Manual. East Aurora, NY: Slosson Educational Publications.
-
- American Psychiatric Association [APA] (2000). Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), 4th Edn. Washington, DC: American Psychiatric Association.
-
- American Psychiatric Association [APA] (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-V), 5th Edn. Washington, DC: American Psychiatric Association; 10.1176/appi.books.9780890425596 - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical