

Blood Shift During Cough: Negligible or Significant?
- PMID: 29892226
- PMCID: PMC5985436
- DOI: 10.3389/fphys.2018.00501
Blood Shift During Cough: Negligible or Significant?
Abstract
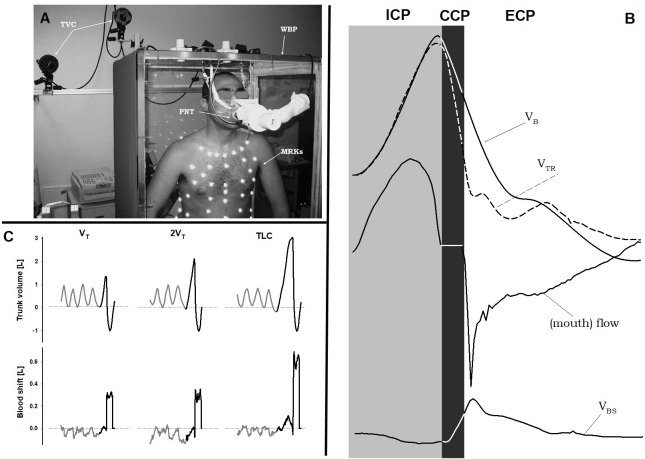
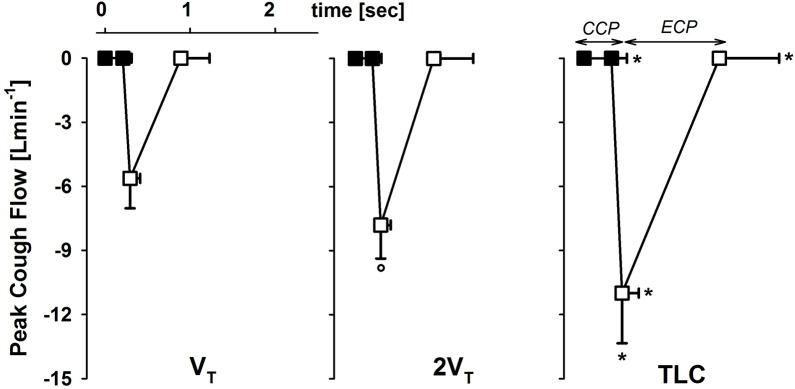
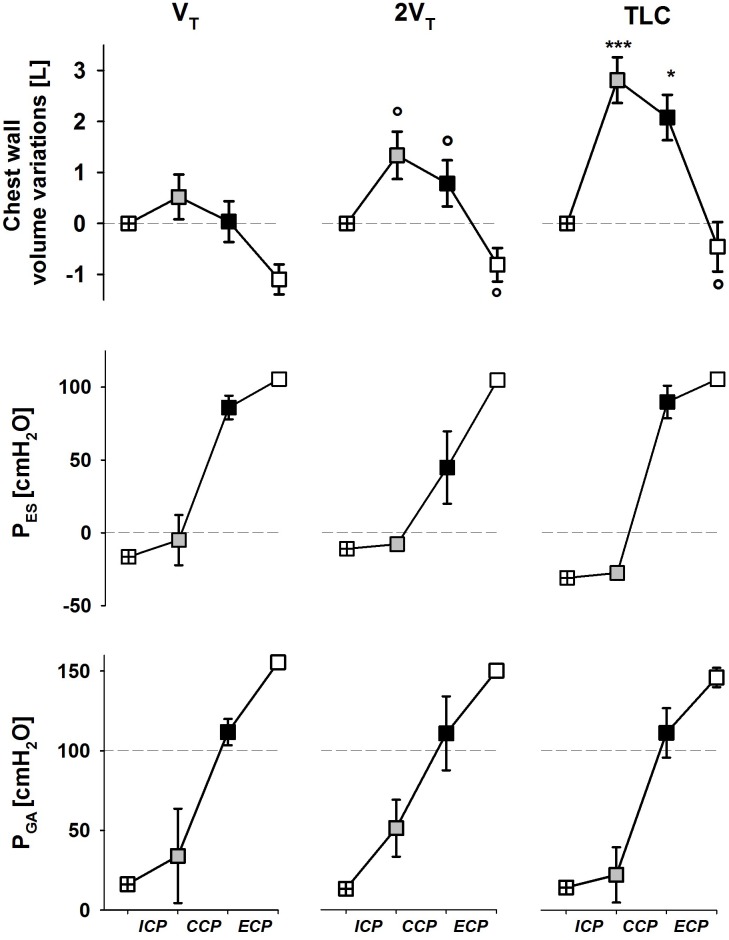
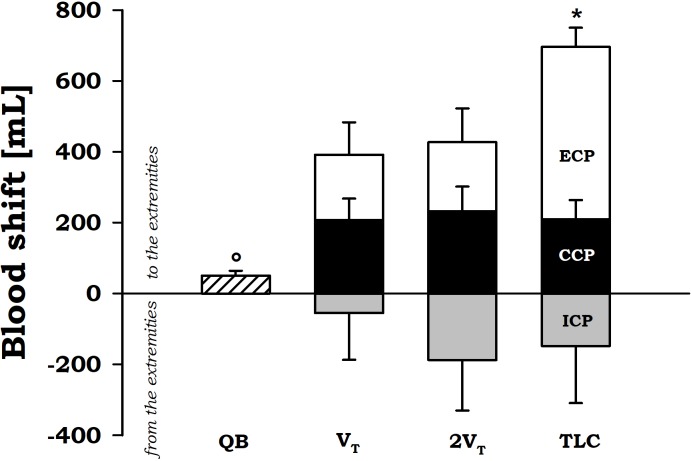
Rationale: It was reported how forceful rhythmic coughing can provide effective blood flow during ventricular fibrillation without direct chest compression. This mechanism of cough-assisted cardiopulmonary resuscitation constitutes a form of "cardiac massage" secondary to the intrathoracic and intra-abdominal pressure changes during cough. We have previously shown that significant blood shifts (BSs) occurs from the thorax to the extremities during expulsive maneuvers and that abdominal pressure controls the outflow of blood from the splanchnic vasculature. This mechanism was called abdominal circulatory pump. BS was quantified by using double body plethysmography (DBP), which combines total body plethysmography and opto-electronic plethysmography. Aim: We hypothesized that coughing activates also the abdominal circulatory pump, being an additional mechanism that displaces a circulatory output sufficient to maintain consciousness in a patient with a non-beating heart. Methods and Results: We studied seven healthy subjects (age: 28.6 ± 2.5 years) during series of voluntary coughs at three different operating volumes: after a spontaneous tidal volume, at total lung capacity (TLC) and at an intermediate volume. BS from the thorax to the extremities were measured by DBP during quiet breathing and during cough at each operating lung volume. BS during cough resulted significantly higher than during quiet breathing (p < 0.05). During the compressive phase, the blood outflow is around 200 ml, whereas during the expulsive phase BS increased (p < 0.05) with increasing operating volume, being almost 700 ml at TLC. At lower operating volume it is almost 400 ml. Conclusion: Deep, vigorous coughing and the consequent fluctuations in intra-thoracic and intra-abdominal pressure activate both the thoracic and the abdominal pump mechanism. The former leads the low-resistance pulmonary veins to empty into the left heart. The latter can generate a circulatory output from the splanchnic region, which acts as a blood reservoir, to other body tissues. These findings might help to better understand the cardiopulmonary interactions during cough, particularly in patients with unstable cardiac function, and the mechanism by which coughing during unstable cardiac rhythms can maintain consciousness in human subjects.
Keywords: blood flow; cardiopulmonary resuscitation; cough; double body plethysmography; physiology.
Figures
References
-
- American Heart Association (2018). Cough CPR. Available at: http://www.heart.org/HEARTORG/Conditions/More/CardiacArrest/Cough-CPR_UC... [Accessed March 20, 2018].
LinkOut - more resources
Full Text Sources
Other Literature Sources