

One-year Outcomes in Patients with ST-segment Elevation Myocardial Infarction Caused by Unprotected Left Main Coronary Artery Occlusion Treated by Primary Percutaneous Coronary Intervention
- PMID: 29893357
- PMCID: PMC6006809
- DOI: 10.4103/0366-6999.233948
One-year Outcomes in Patients with ST-segment Elevation Myocardial Infarction Caused by Unprotected Left Main Coronary Artery Occlusion Treated by Primary Percutaneous Coronary Intervention
Abstract
Background: Very few data have been reported for ST-segment elevation myocardial infarction (STEMI) caused by unprotected left main coronary artery (ULMCA) occlusion, and very little is known about the results of this subgroup of patients who underwent primary percutaneous coronary intervention (PCI). The aim of this study was to determine the clinical features and outcomes of patients with STEMI who underwent primary PCI for acute ULMCA occlusion.
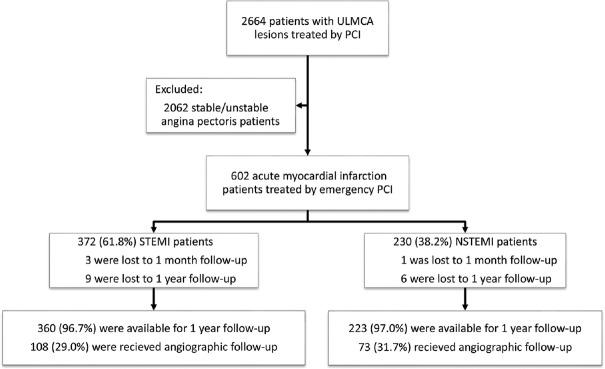
Methods: From January 2000 to February 2014, 372 patients with STEMI caused by ULMCA acute occlusion (ULMCA-STEMI) who underwent primary PCI at one of two centers were enrolled. The 230 patients with non-ST-segment elevation MI (NSTEMI) caused by ULMCA lesion (ULMCA-NSTEMI) who underwent emergency PCI were designated the control group. The main indexes were the major adverse cardiac events (MACEs) in-hospital, at 1 month, and at 1 year.
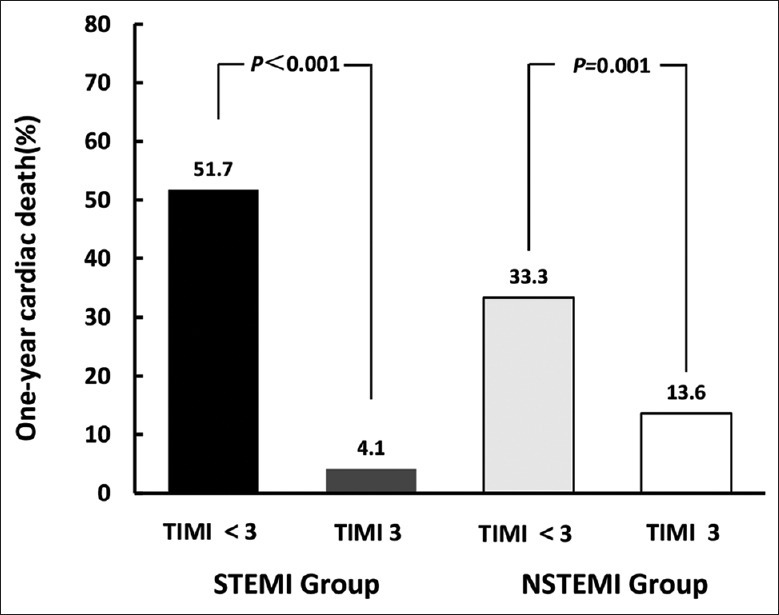
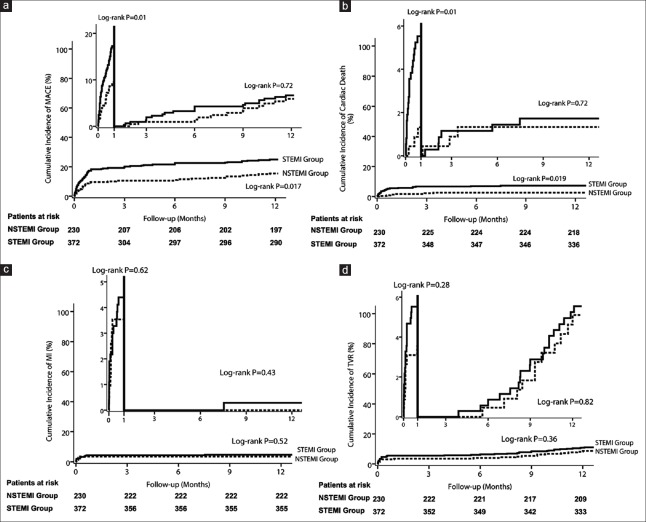
Results: Compared to the NSTEMI patients, the patients with STEMI had significantly higher rates of Killip class≥III (21.2% vs. 3.5%, χ2 = 36.253, P < 0.001) and cardiac arrest (8.3% vs. 3.5%, χ2 = 5.529, P = 0.019). For both groups, the proportions of one-year cardiac death in the patients with a post-procedure thrombolysis in myocardial infarction (TIMI) flow grade<3 were significantly higher than those in the patients with a TIMI flow grade of 3 (STEMI group: 51.7% [15/29] vs. 4.1% [14/343], P < 0.001; NSTEMI group: 33.3% [3/9] vs. 13.6% [3/221], P = 0.001; respectively]. Landmark analysis showed that the patients in STEMI group were associated with higher risks of MACE (16.7% vs. 9.1%, P = 0.009) and cardiac death (5.4% vs. 1.3%, P = 0.011) compared with NSTEMI patients at 1 month. Meanwhile, in patients with ULMCA, the landmark analysis for incidences of MACE and cardiac death was similar between the STEMI and NSTEMI (all P = 0.72) in the intervals of 1-12 months. However, patients who were diagnosed with STEMI or NSTEMI had no significant difference in reinfarction (all P > 0.05) and TVR (all P > 0.05) in the intervals of 0-1 month as well as 1 month to 1 year. The results of Cox regression analysis showed that the differences in the independent predictors for MACE included the variables of Killip class ≥ III and intra-aortic balloon pump support for the STEMI patients and the variables of previous MI, ULMCA distal bifurcation, and 2-stent for distal ULMCA lesions for the NSTEMI patients.
Conclusions: Compared to the NSTEMI patients, the patients with STEMI and ULMCA lesions still remain at a much higher risk for adverse events at 1 year, especially on 1 month. If a successful PCI procedure is performed, the 1-year outcomes in those patients might improve.
直接PCI治疗无保护左主干闭塞所致ST段抬高型心肌梗死的1年疗效观察摘要背景: 目前关于直接经皮冠状动脉介入(PCI)治疗无保护左主干(ULMCA)闭塞所致ST段抬高型心肌梗死(STEMI)患者疗效的相关研究报道非常少。本文旨在观察直接PCI治疗ULMCA为罪犯病变STEMI患者的临床特点及预后。 方法: 在2000.1~2014.2期间,沈阳军区总医院和南京第一医院心脏中心共有372例ULMCA闭塞导致的STEMI患者(ULMCA-STEMI)接受了直接PCI治疗。另有230例ULMCA病变导致非ST段抬高型心肌梗死患者(ULMCA-NSTEMI)接受了急诊PCI,此部分患者设为对照组。主要观察终点为患者住院期间、1个月及1年的主要心脏不良事件[MACE,包括心性死亡、心肌梗死(MI)及靶血管重建(TVR)]。 结果: 分析提示,Killip≥Ⅲ级和有心脏复苏史的患者在STEMI组的比例明显高于NSTEMI组(分别是21.2% vs. 3.5%, χ2 = 36.253, P<0.001和8.3% vs. 3.5%, χ2 = 5.529, P=0.019)。亚组分析结果提示,两组术后血流TIMI<3级患者的1年心性死亡率均明显高于术后血流TIMI 3级的患者(分别是STEMI组: 51.7% [15/29] vs. 4.1% [14/343], P<0.001; NSTEMI组: 33.3% [3/9] vs. 13.6% [3/221], P=0.001)。Landmark分析显示与NSTEMI患者相比,STEMI组患者术后1个月内具有更高的MACE和心性死亡风险(分别是P=0.009;P=0.011),但在术后1个月至12个月期间,两组MACE和心性死亡的风险无明显差异(均P=0.72)。无论在术后1个月内还是在术后1个月至12个月期间,两组再发MI和TVR的风险无明显差异(均P>0.05)。Cox回归分析显示,两组患者发生MACE的独立危险因素存在不同,其中Killip≥Ⅲ级和置入主动脉内囊反搏是STEMI组患者发生MACE的独立危险因素, 而既往MI、分叉病变及双支架术是NSTEMI组患者发生MACE的独立危险因素。 结论: 与NSTEMI患者相比,因ULMCA急性闭塞的STEMI患者术后仍然面临较高的1年心脏事件风险,尤其是在术后1个月内更甚。无论STMEI还是NSTEMI患者,若PCI手术成功实施,均将改善其1年的临床疗效。.
Keywords: Left Main Coronary Artery; Myocardial Infarction; Percutaneous Coronary Intervention.
Conflict of interest statement
There are no conflicts of interest
Figures
References
-
- Gagnor A, Tomassini F, Romagnoli E, Infantino V, Rosa Brusin MC, Maria C, et al. Percutaneous left main coronary disease treatment without on-site surgery back-up in patients with acute coronary syndromes. Catheter Cardiovasc Interv. 2011;79:979–87. doi: 10.1002/ccd.23225. - PubMed
-
- Lee MS, Bokhoor P, Park SJ, Kim YH, Stone GW, Sheiban I, et al. Unprotected left main coronary disease and ST-segment elevation myocardial infarction: A contemporary review and argument for percutaneous coronary intervention. JACC Cardiovasc Interv. 2010;3:791–5. doi: 10.1016/j.jcin.2010.06.005. - PubMed
-
- Pedrazzini GB, Radovanovic D, Vassalli G, Sürder D, Moccetti T, Eberli F, et al. Primary percutaneous coronary intervention for unprotected left main disease in patients with acute ST-segment elevation myocardial infarction the AMIS (Acute myocardial infarction in Switzerland) plus registry experience. JACC Cardiovasc Interv. 2011;4:627–33. doi: 10.1016/j.jcin.2011.04.004. - PubMed
-
- Pappalardo A, Mamas MA, Imola F, Ramazzotti V, Manzoli A, Prati F, et al. Percutaneous coronary intervention of unprotected left main coronary artery disease as culprit lesion in patients with acute myocardial infarction. JACC Cardiovasc Interv. 2011;4:618–26. doi: 10.1016/j.jcin.2011.02.016. - PubMed
-
- Izumikawa T, Sakamoto S, Takeshita S, Takahashi A, Saito S. Outcomes of primary percutaneous coronary intervention for acute myocardial infarction with unprotected left main coronary artery occlusion. Catheter Cardiovasc Interv. 2012;79:1111–6. doi: 10.1002/ccd.23396. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
