

Quadriceps Neuromuscular Function in Patients With Anterior Cruciate Ligament Reconstruction With or Without Knee Osteoarthritis: A Cross-Sectional Study
- PMID: 29893603
- PMCID: PMC6107773
- DOI: 10.4085/1062-6050-102-17
Quadriceps Neuromuscular Function in Patients With Anterior Cruciate Ligament Reconstruction With or Without Knee Osteoarthritis: A Cross-Sectional Study
Abstract
Context: Central and peripheral neural adaptations have been identified after anterior cruciate ligament (ACL) injury and reconstruction (ACLR) and are hypothesized to contribute to posttraumatic muscle dysfunction. Limited evidence exists about the temporal nature of neuromuscular adaptations during early and late-term phases of recovery after ACLR, and no researchers have studied patients with posttraumatic osteoarthritis.
Objective: To compare quadriceps neuromuscular function less than 2 years ( early) and more than 2 years ( late) after ACLR, including in patients who experienced posttraumatic knee osteoarthritis.
Design: Cross-sectional study.
Setting: Laboratory.
Patients or other participants: A total of 72 patients after ACLR, consisting of 34 early (9.0 ± 4.3 months postsurgery), 30 late (70.5 ± 41.6 months postsurgery), and 8 with osteoarthritis (115.9 ± 110.0 months postsurgery), and 30 healthy control volunteers.
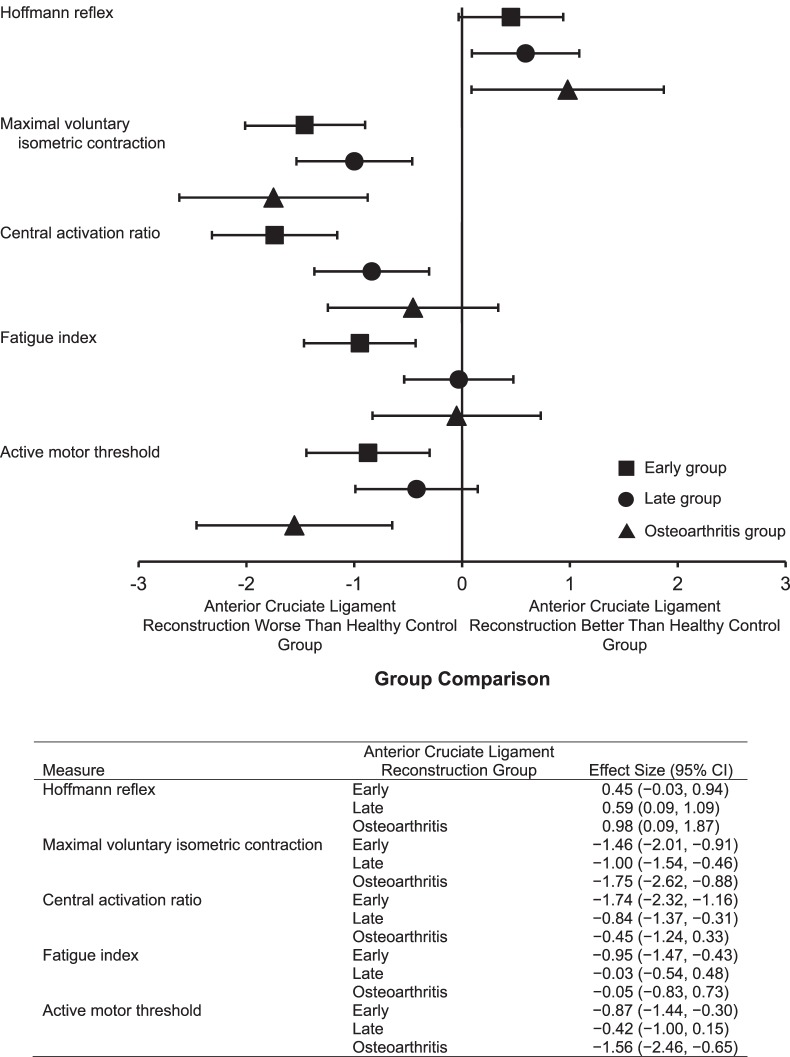
Main outcome measure(s): Quadriceps function was measured bilaterally during a single visit to determine normalized Hoffmann reflex (H : M ratio), knee-extension maximal voluntary isometric contraction torque (Nm/kg), central activation ratio (%), fatigue index (% decline), and active motor threshold (%). Comparisons were made using 2-way analyses of variance to identify the effect of limb and group on each outcome measure. We calculated Cohen d effect sizes to assess the magnitude of difference between ACLR and matched control limbs for each group.
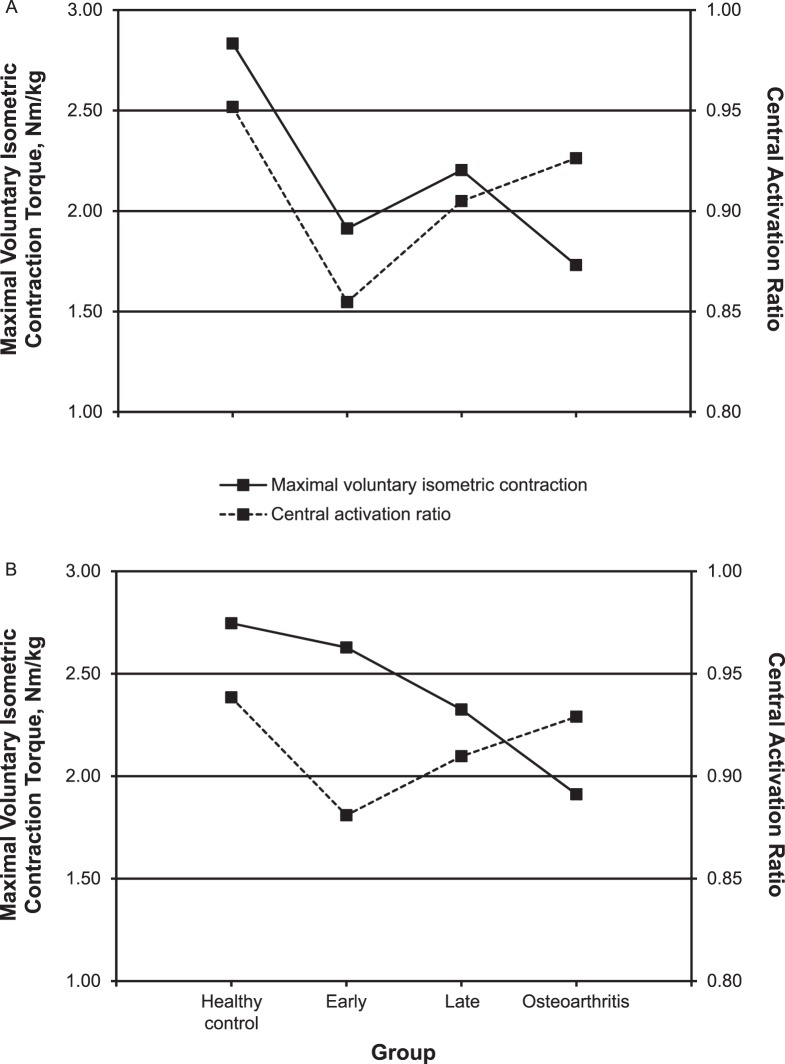
Results: Compared with healthy control limbs, involved-limb maximal voluntary isometric contraction was lower among all patients after ACLR ( P < .001, Cohen d values = -1.00 to -1.75). The central activation ratio ( P < .001, Cohen d = -1.74) and fatigue index ( P = .003, Cohen d = -0.95) were lower among patients only early after ACLR. The active motor threshold was higher among all patients after ACLR ( P < .001, Cohen d values = -0.42 to -1.56).
Conclusions: Neuromuscular impairments were present in patients early and late after ACLR, regardless of osteoarthritis status. Quadriceps strength and corticospinal excitability were impaired at each time point compared with values in healthy control individuals, suggesting the need to address cortical function early after ACLR.
Keywords: corticospinal excitability; muscle activation; spinal-reflex excitability.
Figures
References
-
- Ardern CL, Taylor NF, Feller JA, Webster KE. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br J Sports Med. 2014;48(21):1543–1552. - PubMed
-
- Oiestad BE, Juhl CB, Eitzen I, Thorlund JB. Knee extensor muscle weakness is a risk factor for development of knee osteoarthritis: a systematic review and meta-analysis. Osteoarthritis Cartilage. 2015;23(2):171–177. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
