

Vancomycin Monotherapy May Be Insufficient to Treat Methicillin-resistant Staphylococcus aureus Coinfection in Children With Influenza-related Critical Illness
- PMID: 29893805
- PMCID: PMC6336914
- DOI: 10.1093/cid/ciy495
Vancomycin Monotherapy May Be Insufficient to Treat Methicillin-resistant Staphylococcus aureus Coinfection in Children With Influenza-related Critical Illness
Abstract
Background: Coinfection with influenza virus and methicillin-resistant Staphylococcus aureus (MRSA) causes life-threatening necrotizing pneumonia in children. Sporadic incidence precludes evaluation of antimicrobial efficacy. We assessed the clinical characteristics and outcomes of critically ill children with influenza-MRSA pneumonia and evaluated antibiotic use.
Methods: We enrolled children (<18 years) with influenza infection and respiratory failure across 34 pediatric intensive care units 11/2008-5/2016. We compared baseline characteristics, clinical courses, and therapies in children with MRSA coinfection, non-MRSA bacterial coinfection, and no bacterial coinfection.
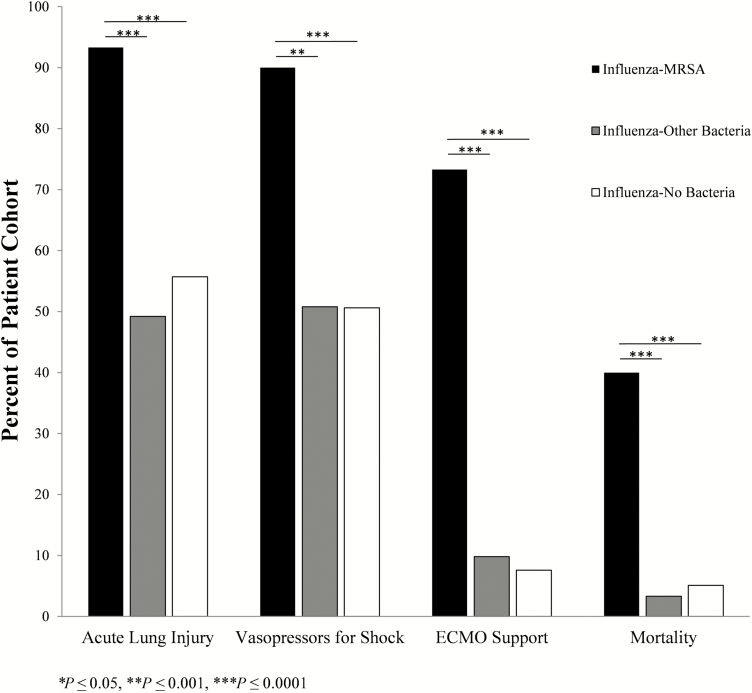
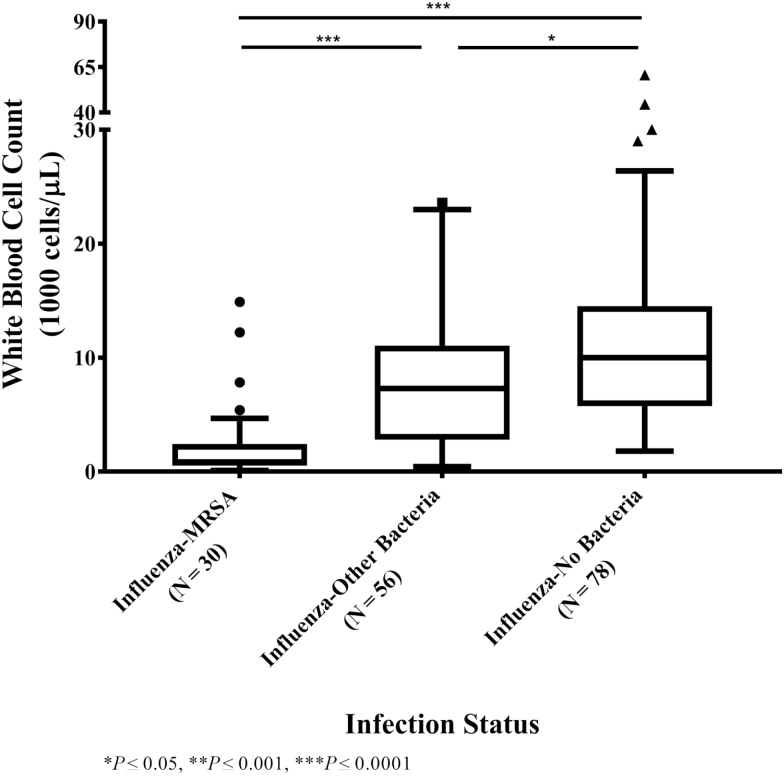
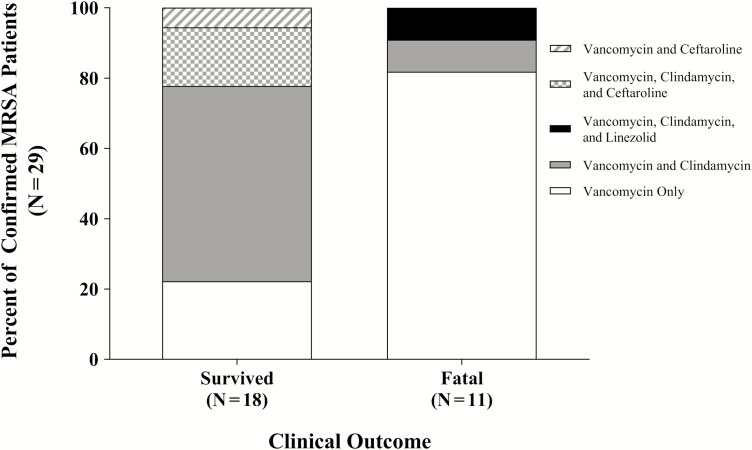
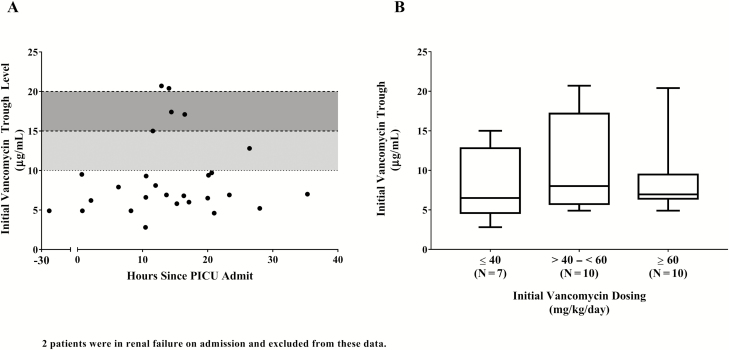
Results: We enrolled 170 children (127 influenza A, 43 influenza B). Children with influenza-MRSA pneumonia (N = 30, 87% previously healthy) were older than those with non-MRSA (N = 61) or no (N = 79) bacterial coinfections. Influenza-MRSA was associated with increased leukopenia, acute lung injury, vasopressor use, extracorporeal life support, and mortality than either group (P ≤ .0001). Influenza-related mortality was 40% with MRSA compared to 4.3% without (relative risk [RR], 9.3; 95% confidence interval [CI], 3.8-22.9). Of 29/30 children with MRSA who received vancomycin within the first 24 hours of hospitalization, mortality was 12.5% (N = 2/16) if treatment also included a second anti-MRSA antibiotic compared to 69.2% (N = 9/13) with vancomycin monotherapy (RR, 5.5; 95% CI, 1.4, 21.3; P = .003). Vancomycin dosing did not influence initial trough levels; 78% were <10 µg/mL.
Conclusions: Influenza-MRSA coinfection is associated with high fatality in critically ill children. These data support early addition of a second anti-MRSA antibiotic to vancomycin in suspected severe cases.
Figures
Comment in
-
The Concern for Vancomycin Failure in the Treatment of Pediatric Staphylococcus aureus Disease.Clin Infect Dis. 2019 Jan 18;68(3):373-374. doi: 10.1093/cid/ciy497. Clin Infect Dis. 2019. PMID: 29893812 Free PMC article. No abstract available.
References
-
- Reed C, Kallen AJ, Patton M, et al. . Infection with community-onset Staphylococcus aureus and influenza virus in hospitalized children. Pediatr Infect Dis J 2009; 28:572–6. - PubMed
-
- Centers for Disease Control and Prevention. Severe methicillin-resistant Staphylococcus aureus community-acquired pneumonia associated with influenza—Louisiana and Georgia, December 2006-January 2007. MMWR Morb Mortal Wkly Rep 2007; 56:325–9. - PubMed
-
- Finelli L, Fiore A, Dhara R, et al. . Influenza-associated pediatric mortality in the United States: increase of Staphylococcus aureus coinfection. Pediatrics 2008; 122:805–11. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
