

Indirect neonatal hyperbilirubinemia in hospitalized neonates on the Thai-Myanmar border: a review of neonatal medical records from 2009 to 2014
- PMID: 29895274
- PMCID: PMC5998587
- DOI: 10.1186/s12887-018-1165-0
Indirect neonatal hyperbilirubinemia in hospitalized neonates on the Thai-Myanmar border: a review of neonatal medical records from 2009 to 2014
Abstract
Background: Indirect neonatal hyperbilirubinemia (INH) is a common neonatal disorder worldwide which can remain benign if prompt management is available. However there is a higher morbidity and mortality risk in settings with limited access to diagnosis and care. The manuscript describes the characteristics of neonates with INH, the burden of severe INH and identifies factors associated with severity in a resource-constrained setting.
Methods: We conducted a retrospective evaluation of anonymized records of neonates hospitalized on the Thai-Myanmar border. INH was defined according to the National Institute for Health and Care Excellence guidelines as 'moderate' if at least one serum bilirubin (SBR) value exceeded the phototherapy threshold and as 'severe' if above the exchange transfusion threshold.
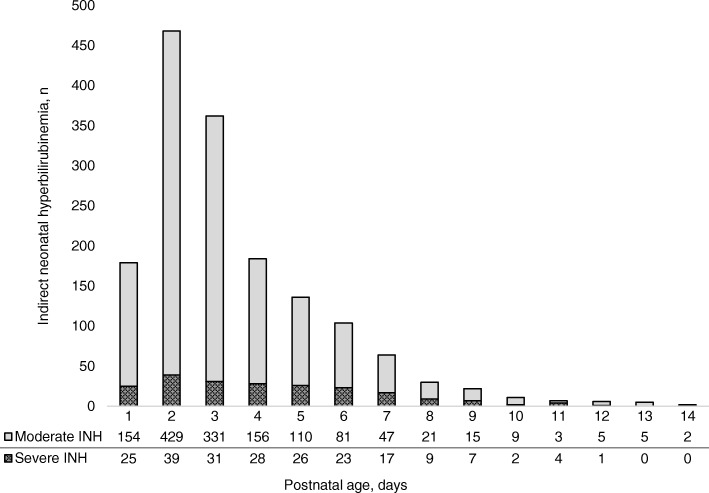
Results: Out of 2980 records reviewed, 1580 (53%) had INH within the first 14 days of life. INH was moderate in 87% (1368/1580) and severe in 13% (212/1580). From 2009 to 2011, the proportion of severe INH decreased from 37 to 15% and the mortality dropped from 10% (8/82) to 2% (7/449) coinciding with the implementation of standardized guidelines and light-emitting diode (LED) phototherapy. Severe INH was associated with: prematurity (< 32 weeks, Adjusted Odds Ratio (AOR) 3.3; 95% CI 1.6-6.6 and 32 to 37 weeks, AOR 2.2; 95% CI 1.6-3.1), Glucose-6-phosphate dehydrogenase deficiency (G6PD) (AOR 2.3; 95% CI 1.6-3.3), potential ABO incompatibility (AOR 1.5; 95% CI 1.0-2.2) and late presentation (AOR 1.8; 95% CI 1.3-2.6). The risk of developing severe INH and INH-related mortality significantly increased with each additional risk factor.
Conclusion: INH is an important cause of neonatal hospitalization on the Thai-Myanmar border. Risk factors for severity were similar to previous reports from Asia. Implementing standardized guidelines and appropriate treatment was successful in reducing mortality and severity. Accessing to basic neonatal care including SBR testing, LED phototherapy and G6PD screening can contribute to improve neonatal outcomes.
Keywords: (LED-) phototherapy; Indirect neonatal hyperbilirubinemia; Jaundice; Low-resource; Migrant; Mortality; Neonates; Refugee; Resource-limited setting.
Conflict of interest statement
Ethics approval and consent to participate
This retrospective analysis of anonymized data was exempted from formal ethical review (confirmed by Oxford Tropical Research Ethics Committee (OxTREC) on February 2017) and discussed with the Tak Province Border Community Ethics Advisory Board (T-CAB-01/FEV/2017). The retrospective anonymized dataset made the requirement for individual informed consent not applicable for this study.
Competing interests
All authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Radmacher PG, Groves FD, Owa JA, Ofovwe GE, Amuabunos EA, Olusanya BO, et al. A modified bilirubin-induced neurologic dysfunction (BIND-M) algorithm is useful in evaluating severity of jaundice in a resource-limited setting. BMC Pediatr. 2015;15:1–7. doi: 10.1186/s12887-015-0355-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
