

Improvement in the active management of the third stage of labor for the prevention of postpartum hemorrhage in Tanzania: a cross-sectional study
- PMID: 29895276
- PMCID: PMC5998542
- DOI: 10.1186/s12884-018-1873-3
Improvement in the active management of the third stage of labor for the prevention of postpartum hemorrhage in Tanzania: a cross-sectional study
Abstract
Background: Tanzania has a maternal mortality ratio of 556 per 100,000 live births, representing 21% of all deaths of women of reproductive age. Hemorrhage, mostly postpartum hemorrhage (PPH), is estimated to cause at least 25% of maternal deaths in Tanzania. In 2008, the Ministry of Health, Community Development, Gender, Elderly and Children launched interventions to improve efforts to prevent PPH. Competency-based training for skilled birth attendants and ongoing quality improvement prioritized the practice of active management of the third stage of labor (AMTSL).
Methods: A cross-sectional study was conducted in 52 health facilities in Tanzania utilizing direct observations of women during labor and delivery. Observations were conducted in 2010 and, after competency-based training and quality improvement interventions in the facilities, in 2012. A total of 489 deliveries were observed in 2010 and 558 in 2012. Steps for AMTSL were assessed using a standardized structured observation checklist that was based on World Health Organization guidelines.
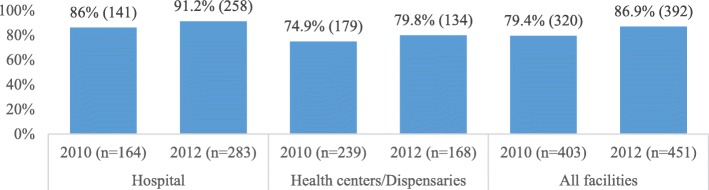
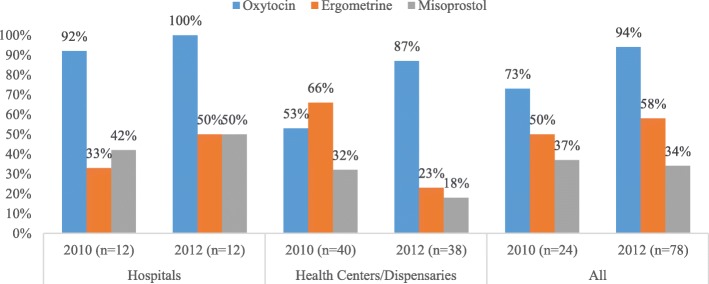
Results: The proportion of deliveries receiving all three AMTSL steps improved significantly by 19 percentage points (p < 0.001) following the intervention, with the most dramatic increase occurring in health centers and dispensaries (47.2 percentage point change) compared to hospitals (5.2 percentage point change). Use of oxytocin for PPH prevention rose by 37.1 percentage points in health centers and dispensaries but remained largely the same in hospitals, where the baseline was higher. There was substantial improvement in the timely provision of uterotonics (within 3 min of birth) across all facilities (p = 0.003). Availability of oxytocin, which was lower in health centers and dispensaries than hospitals at baseline, rose from 73 to 94% of all facilities.
Conclusion: The quality of PPH prevention increased substantially in facilities that implemented competency-based training and quality improvement interventions, with the most dramatic improvement seen at lower-level facilities. As Tanzania continues with efforts to increase facility births, it is imperative that the quality of care also be improved by promoting use of up-to-date guidelines and ensuring regular training and mentoring for health care providers so that they adhere to the guidelines for care of women during labor. These measures can reduce maternal and newborn mortality.
Keywords: AMTSL; Active management of the third stage of labor; Obstetric complications; Postpartum hemorrhage; Quality of care; Tanzania; Uterotonic.
Conflict of interest statement
Ethics approval and consent to participate
Ethical clearance was obtained from the Ethical Review Board of the Tanzania National Institute of Medical Research (Reference No. NIMR/HQ/R.8C/Vol II/164) and the Johns Hopkins Bloomberg School of Public Health Institutional Review Board (IRB No. 00002549). Written consent was obtained from facility directors or maternity unit in-charges to observe quality of care in the facility. Verbal consent was obtained from women observed. Both consent forms were approved by IRBs overseeing the study. The clinical observer recorded verbal consents of women observed in the mobile device. In all cases, neither the names or personal identifiers were recorded.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- World Bank . Trends in Maternal Mortality: 1990 to 2015—estimates by WHO, UNICEF, UNFPA, the World Bank Group, and the United Nations population division. Washington DC: World Bank Group; 2010.
-
- Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) [Tanzania Mainland], Ministry of Health Zanzibar, National Bureua of Statistics (NBS), Office of Chief Government Statitician, ICF . Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2015–16. Dar es Salaam, Tanzania, and Rockville, MD, USA: MoHCDGEC, MoH, NBS, OCGS, and ICF; 2016. pp. 172–173.
-
- NBS and ICF Macro. Tanzania Demographic and Health Survey 2010. Dar es Salaam: NBS and ICF Macro; 2011.
-
- NBS and ORC Macro . Tanzania Demographic and Health Survey 2004–05. Dar es Salaam, Tanzania: NBS and ORC Macro; 2005.
-
- World Health Organization (WHO) Standards for improving quality of maternal and newborn care in health facilities. Geneva: WHO; 2016. p. 73.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
