

Effectiveness of motivational interviewing, health education and brief advice in a population of smokers who are not ready to quit
- PMID: 29895280
- PMCID: PMC5998452
- DOI: 10.1186/s12874-018-0511-0
Effectiveness of motivational interviewing, health education and brief advice in a population of smokers who are not ready to quit
Abstract
Background: Motivational Interviewing (MI), Brief Advice (BA) and Health Education (HE) are established smoking cessation induction methods for smokers with low desire to quit. Although randomized controlled trials (RCT's) have been frequently used to assess these interventions the temporal efficacy and effectiveness of these interventions have been poorly elaborated. The present work endeavors to fill the gap by considering the full range of possible motivational outcomes for all of the participants.
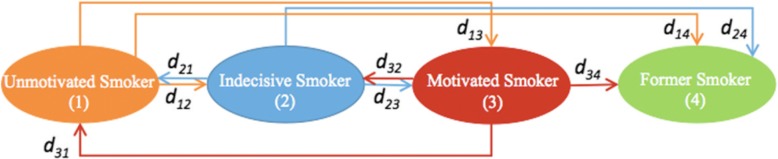
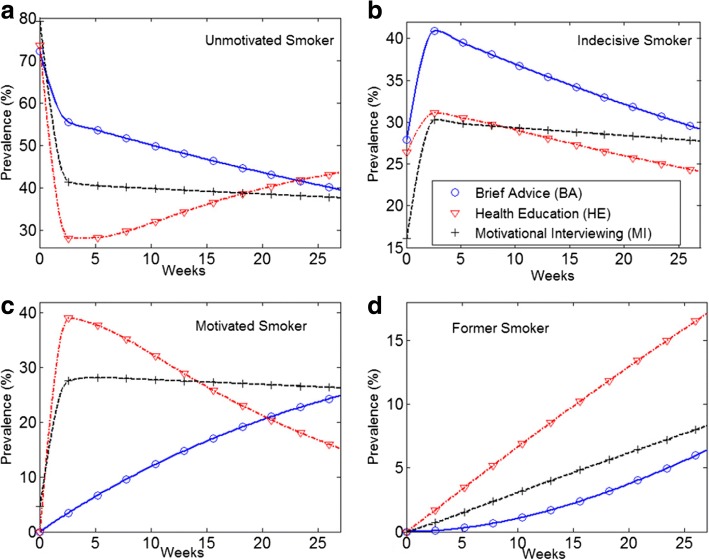
Methods: As a two-step process, Markov Chain (MC) and Ordinary Differential Equation (ODE) models were successively employed to examine the temporal efficacy and effectiveness of these interventions by computing the gradual movements of participants from an initial stage of unmotivated smoker to stages of increased motivation to quit and cessation. Specifically, in our re-analysis of data from the RCT we examined the proportion of participants in 4 stages of readiness to quit (unmotivated, undecided, motivated, former smokers) over 6 months, across treatment groups [MI (n = 87), BA (n = 43) and HE (n = 91)].
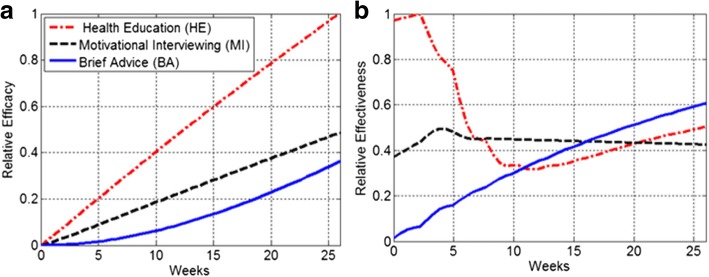
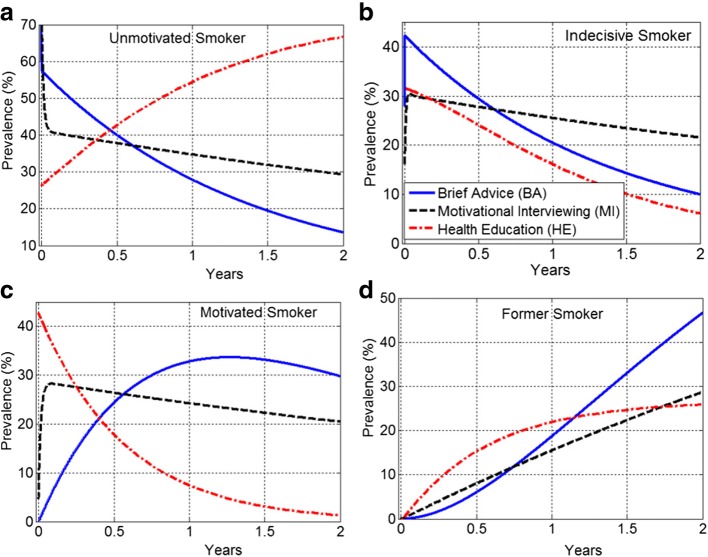
Results: Although HE had greater efficacy compared to MI and BA (i.e., the highest smoking cessation rates), it had lower effectiveness at certain time points. This was due to the fact that HE had the greatest proportion of motivated smokers who quit smoking but simultaneously a large proportion of the motivated smokers became unmotivated to quit. The effectiveness of HE dropped substantially in weeks 3-12 and remained below the effectiveness of BA from week 12 onward. The 2-year ODE model projections show that the prevalence of motivated smokers in HE group may fall below 5%. The prevalence of HE former smokers can reach an equilibrium of 26%, where the prevalence of both BA and MI former smokers exceeds this equilibrium.
Conclusions: The methodology proposed in this paper strongly benefits from the capabilities of both MC and ODE modeling approaches, in the event of low observations over the time. Particularly, the temporal population sizes are first estimated by the MC model. Then they are used to parametrize the ODE model and predict future values. The methodology enabes us to determine and compare the temporal efficacy and effectiveness of smoking cessation interventions, yielding predictive and analytic insights related to temporal characteristics and capabilities of these interventions during the study period and beyond.
Trial registration: Testing Counseling Styles to Motivate Smokers to Quit, NCT01188018 , (July 4, 2012). This study is registered at www.clinicaltrials.gov NCT01188018.
Keywords: Brief advice; Effectiveness; Efficacy; Health education; Markov chain model; Motivational interviewing; Smoking cessation.
Conflict of interest statement
Ethics approval and consent to participate
UMKC Adult Health Sciences IRB Protocol #: 09–78. The consent to participate was obtained from all participants and it was in written format.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
