

Immunocompromised patients with acute respiratory distress syndrome: secondary analysis of the LUNG SAFE database
- PMID: 29895331
- PMCID: PMC5998562
- DOI: 10.1186/s13054-018-2079-9
Immunocompromised patients with acute respiratory distress syndrome: secondary analysis of the LUNG SAFE database
Abstract
Background: The aim of this study was to describe data on epidemiology, ventilatory management, and outcome of acute respiratory distress syndrome (ARDS) in immunocompromised patients.
Methods: We performed a post hoc analysis on the cohort of immunocompromised patients enrolled in the Large Observational Study to Understand the Global Impact of Severe Acute Respiratory Failure (LUNG SAFE) study. The LUNG SAFE study was an international, prospective study including hypoxemic patients in 459 ICUs from 50 countries across 5 continents.
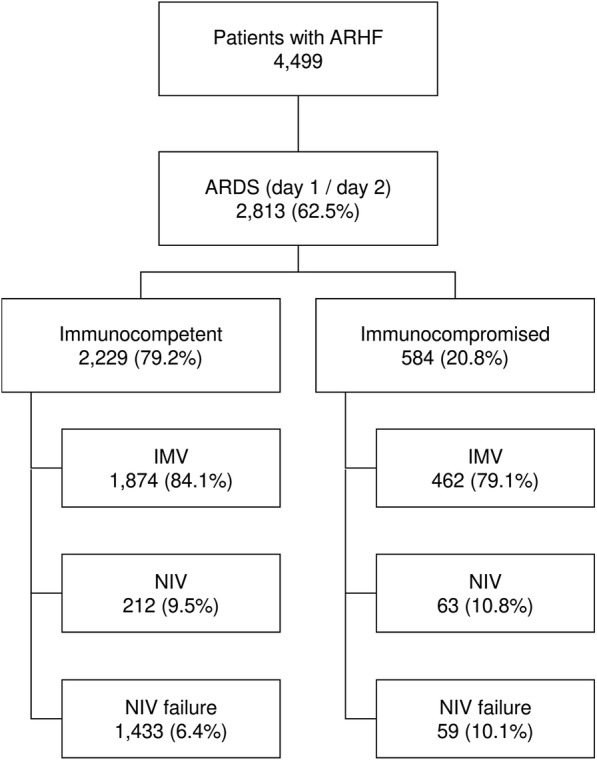
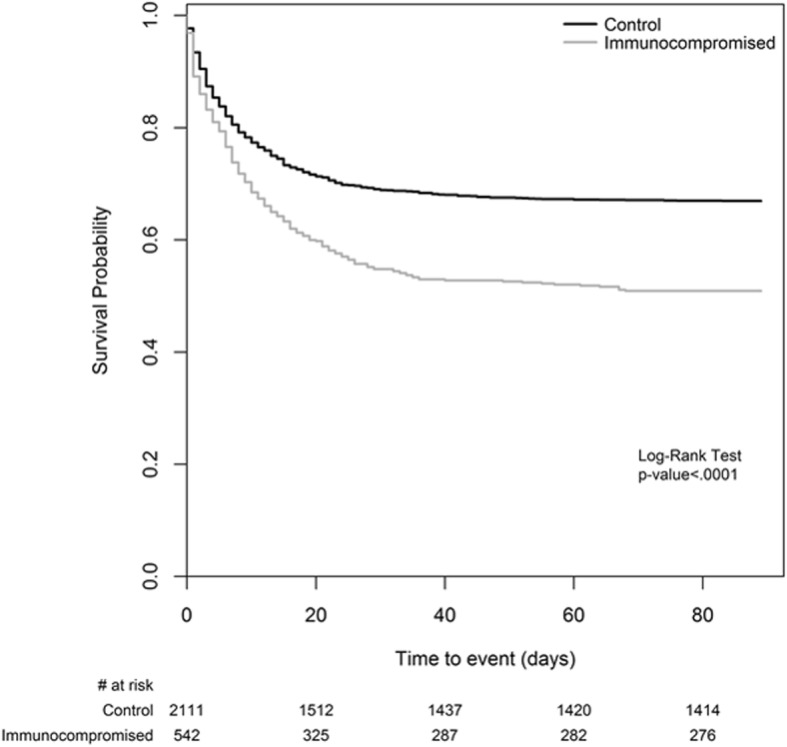
Results: Of 2813 patients with ARDS, 584 (20.8%) were immunocompromised, 38.9% of whom had an unspecified cause. Pneumonia, nonpulmonary sepsis, and noncardiogenic shock were their most common risk factors for ARDS. Hospital mortality was higher in immunocompromised than in immunocompetent patients (52.4% vs 36.2%; p < 0.0001), despite similar severity of ARDS. Decisions regarding limiting life-sustaining measures were significantly more frequent in immunocompromised patients (27.1% vs 18.6%; p < 0.0001). Use of noninvasive ventilation (NIV) as first-line treatment was higher in immunocompromised patients (20.9% vs 15.9%; p = 0.0048), and immunodeficiency remained independently associated with the use of NIV after adjustment for confounders. Forty-eight percent of the patients treated with NIV were intubated, and their mortality was not different from that of the patients invasively ventilated ab initio.
Conclusions: Immunosuppression is frequent in patients with ARDS, and infections are the main risk factors for ARDS in these immunocompromised patients. Their management differs from that of immunocompetent patients, particularly the greater use of NIV as first-line ventilation strategy. Compared with immunocompetent subjects, they have higher mortality regardless of ARDS severity as well as a higher frequency of limitation of life-sustaining measures. Nonetheless, nearly half of these patients survive to hospital discharge.
Trial registration: ClinicalTrials.gov, NCT02010073 . Registered on 12 December 2013.
Keywords: ARDS; Acute respiratory failure; Immunocompromised patients; Mechanical ventilation; Noninvasive ventilation.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Competing interests
AC, FM, JGL, TP, and FVH declare that they have no competing interests. CG received fees for consultancies or lectures from Orion Pharma, ResMed, Medtronic, Philips, Air Liquide, and EOVE (all unrelated to the present work). GB received fees for lectures from Draeger Medical, GE Healthcare, and Pfizer; research grants from Draeger Medical; and is president and a shareholder of ReviewerCredits S.R.L. (all unrelated to the present work). AG received fees for consultancies or lectures from Orion, Pfizer, and MSD (all unrelated to the present work). MA received research grants from Toray, GE Healthcare, and Orion and participated on the boards and received personal fees from Maquet, Pfizer, and MSD (all unrelated to the present work). AP received fees from Maquet, Novalung, Xenios, Baxter, and Boerhinger Ingelheim (all unrelated to the present work). GG received fees for lectures from Thermo Fisher Scientific and Pfizer and travel accommodation support from Maquet and Biotest (all unrelated to the present work).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Azoulay E, Mokart D, Pene F, Lambert J, Kouatchet A, Mayaux J, Vincent F, Nyunga M, Bruneel F, Laisne L-M, Rabbat A, Lebert C, Perez P, Chaize M, Renault A, Meert A-P, Benoit D, Hamidfar R, Jourdain M, Darmon M, Schlemmer B, Chevret S, Lemiale V. Outcomes of critically ill patients with hematologic malignancies: prospective multicenter data from France and Belgium—a Groupe de Recherche Respiratoire en Reanimation Onco-Hematologique Study. J Clin Oncol. 2013;31:2810–2818. doi: 10.1200/JCO.2012.47.2365. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
