

Pattern and Predictors of Outpatient Palliative Care Referral Among Thoracic Medical Oncologists
- PMID: 29895629
- PMCID: PMC6263132
- DOI: 10.1634/theoncologist.2018-0094
Pattern and Predictors of Outpatient Palliative Care Referral Among Thoracic Medical Oncologists
Abstract
Background: There is significant variation in access to palliative care. We examined the pattern of outpatient palliative care referral among thoracic medical oncologists and identified oncologist characteristics associated with greater referral.
Materials and methods: We retrieved data on all patients who died of advanced thoracic malignancies at our institution between January 1, 2007, and December 31, 2012. Using median as a cutoff, we defined two groups (high-referring and low-referring oncologists) based on their frequency of referral. We examined various oncologist- and patient-related characteristics associated with outpatient referral.
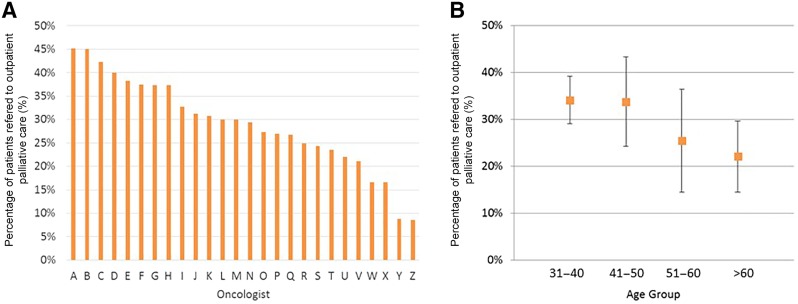
Results: Of 1,642 decedents, 444 (27%) had an outpatient palliative care referral. The median proportion of referral among 26 thoracic oncologists was 30% (range 9%-45%; median proportion of high-referring 37% vs. low-referring 24% when divided into two groups at median). High-referring oncologists were significantly younger (age 45 vs. 56) than low-referring oncologists; they were also significantly more likely to refer patients earlier (median interval between oncology consultation and palliative care consultation 90 days vs. 170 days) and to refer those without metastatic disease (7% vs. 2%). In multivariable mixed-effect logistic regression, younger oncologists (odds ratio [OR] = 0.97 per year increase, 95% confidence interval [CI] 0.95-0.995), younger patients (OR = 0.98 per year increase, 95% CI 0.97-0.99), and nonmetastatic disease status (OR = 0.48, 95% CI 0.29-0.78) were significantly associated with outpatient palliative care referral.
Conclusion: The pattern of referral to outpatient palliative care varied widely among thoracic oncologists. Younger oncologists were not only referring a higher proportion of patients, but also referring patients earlier in the disease trajectory.
Implications for practice: This retrospective cohort study found that younger thoracic medical oncologists were significantly more likely to refer patients to outpatient palliative care and to do so earlier in the disease trajectory compared with older oncologists, even after adjusting for other known predictors such as patient demographics. The findings highlight the role of education to standardize palliative care access and imply that outpatient palliative care referral is likely to continue to increase with a shifting oncology workforce.
Keywords: Ambulatory care; Health knowledge, attitudes, practice; Health services research; Neoplasms; Palliative care; Referral and consultation.
© AlphaMed Press 2018.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
Similar articles
-
Outpatient palliative care and thoracic medical oncology: Referral criteria and clinical care pathways.Lung Cancer. 2020 Jan;139:13-17. doi: 10.1016/j.lungcan.2019.10.003. Epub 2019 Oct 11. Lung Cancer. 2020. PMID: 31704278
-
Gynecologic Oncologist Views Influencing Referral to Outpatient Specialty Palliative Care.Int J Gynecol Cancer. 2017 Mar;27(3):588-596. doi: 10.1097/IGC.0000000000000893. Int J Gynecol Cancer. 2017. PMID: 28060140 Free PMC article.
-
Attitudes and Beliefs Toward Supportive and Palliative Care Referral Among Hematologic and Solid Tumor Oncology Specialists.Oncologist. 2015 Nov;20(11):1326-32. doi: 10.1634/theoncologist.2015-0240. Epub 2015 Sep 28. Oncologist. 2015. PMID: 26417037 Free PMC article.
-
Improving patient and caregiver outcomes in oncology: Team-based, timely, and targeted palliative care.CA Cancer J Clin. 2018 Sep;68(5):356-376. doi: 10.3322/caac.21490. Epub 2018 Sep 13. CA Cancer J Clin. 2018. PMID: 30277572 Free PMC article. Review.
-
How views of oncologists and haematologists impacts palliative care referral: a systematic review.BMC Palliat Care. 2020 Nov 23;19(1):175. doi: 10.1186/s12904-020-00671-5. BMC Palliat Care. 2020. PMID: 33228651 Free PMC article.
Cited by
-
Utilization of palliative care resource remains low, consuming potentially avoidable hospital admissions in stage IV non-small cell lung cancer: a community-based retrospective review.Support Care Cancer. 2022 Dec;30(12):10117-10126. doi: 10.1007/s00520-022-07364-0. Epub 2022 Nov 14. Support Care Cancer. 2022. PMID: 36374328 Free PMC article.
-
Team-Based Hospice Referrals: A Potential Quality Metric for Lung Cancer in the Immunotherapy Era.Am J Hosp Palliat Care. 2023 Jan;40(1):10-17. doi: 10.1177/10499091221091745. Epub 2022 May 5. Am J Hosp Palliat Care. 2023. PMID: 35512681 Free PMC article.
-
Temporal Trends in Opioid Prescribing Patterns Among Oncologists in the Medicare Population.J Natl Cancer Inst. 2021 Mar 1;113(3):274-281. doi: 10.1093/jnci/djaa110. J Natl Cancer Inst. 2021. PMID: 32785685 Free PMC article.
-
Estimated mortality risk and use of palliative care services among home care clients during the last 6 months of life: a retrospective cohort study.CMAJ. 2024 Feb 25;196(7):E209-E221. doi: 10.1503/cmaj.221513. CMAJ. 2024. PMID: 38408785 Free PMC article.
-
Palliative care education and research at US cancer centers: A national survey.Cancer. 2021 Jun 15;127(12):2139-2147. doi: 10.1002/cncr.33474. Epub 2021 Mar 4. Cancer. 2021. PMID: 33662148 Free PMC article.
References
-
- Tishelman C, Petersson LM, Degner LF et al. Symptom prevalence, intensity, and distress in patients with inoperable lung cancer in relation to time of death. J Clin Oncol 2007;25:5381–5389. - PubMed
-
- Temel JS, Jackson VA, Billings JA et al. Phase II study: Integrated palliative care in newly diagnosed advanced non‐small‐cell lung cancer patients. J Clin Oncol 2007;25:2377–2382. - PubMed
-
- Bakitas M, Stevens M, Ahles T et al. Project ENABLE: A palliative care demonstration project for advanced cancer patients in three settings. J Palliat Med 2004;7:363–372. - PubMed
-
- Temel JS, Greer JA, Muzikansky A et al. Early palliative care for patients with metastatic non‐small‐cell lung cancer. N Engl J Med 2010;363:733–742. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
