

A Dual-Modality Hybrid Imaging System Harnesses Radioluminescence and Sound to Reveal Molecular Pathology of Atherosclerotic Plaques
- PMID: 29895966
- PMCID: PMC5997702
- DOI: 10.1038/s41598-018-26696-8
A Dual-Modality Hybrid Imaging System Harnesses Radioluminescence and Sound to Reveal Molecular Pathology of Atherosclerotic Plaques
Abstract
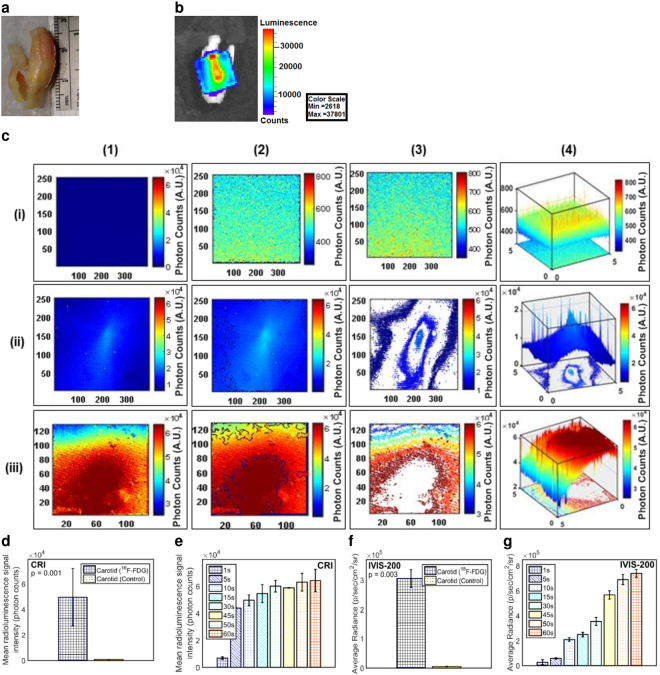
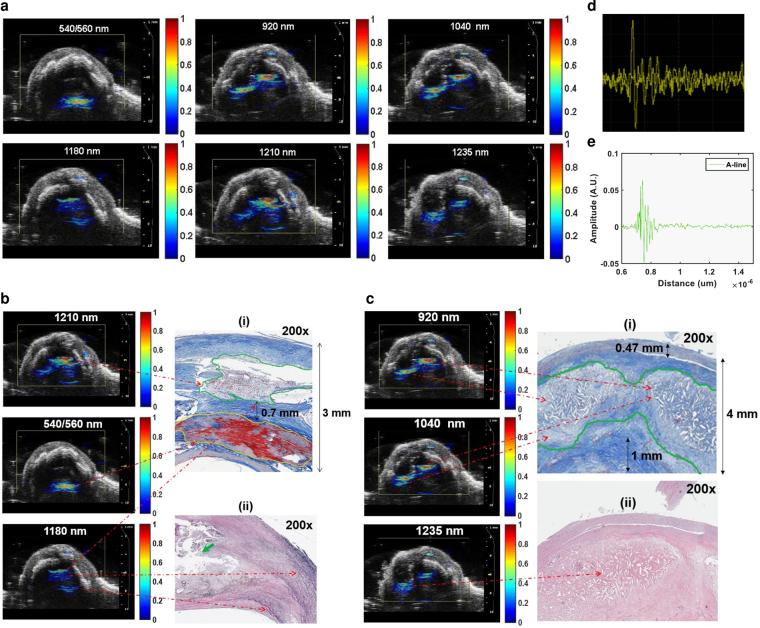
Atherosclerosis is a progressive inflammatory condition caused by an unstable lesion, called thin-cap fibro atheromata (TCFA) that underlies coronary artery disease (CAD)-one of the leading causes of death worldwide. Therefore, early clinical diagnosis and effective risk stratification is important for CAD management as well as preventing progression to catastrophic events. However, early detection could be difficult due to their small size, motion, obscuring 18F-FDG uptake by adjacent myocardium, and complex morphological/biological features. To overcome these limitations, we developed a catheter-based Circumferential-Intravascular-Radioluminescence-Photoacoustic-Imaging (CIRPI) system that can detect vulnerable plaques in coronary arteries and characterizes them with respect to pathology and biology. Our CIRPI system combined two imaging modalities: Circumferential Radioluminescence Imaging (CRI) and PhotoAcoustic Tomography (PAT) within a novel optical probe. The probe's CaF2:Eu based scintillating imaging window provides a 360° view of human (n = 7) and murine carotid (n = 10) arterial plaques by converting β-particles into visible photons during 18F-FDG decay. A 60× and 63× higher radioluminescent signals were detected from the human and murine plaque inflammations, respectively, compared to the control. The system's photoacoustic imaging provided a comprehensive analysis of the plaque compositions and its morphologic information. These results were further verified with IVIS-200, immunohistochemical analysis, and autoradiography.
Conflict of interest statement
Michael V. McConnell is currently a Clinical Professor at the Stanford University School of Medicine and an employee of Verily Life Sciences; however, this does not alter our adherence to the
Figures




Similar articles
-
In Vivo Translation of the CIRPI System: Revealing Molecular Pathology of Rabbit Aortic Atherosclerotic Plaques.J Nucl Med. 2019 Sep;60(9):1308-1316. doi: 10.2967/jnumed.118.222471. Epub 2019 Feb 8. J Nucl Med. 2019. PMID: 30737298 Free PMC article.
-
Fiber-optic system for dual-modality imaging of glucose probes 18F-FDG and 6-NBDG in atherosclerotic plaques.PLoS One. 2014 Sep 18;9(9):e108108. doi: 10.1371/journal.pone.0108108. eCollection 2014. PLoS One. 2014. PMID: 25233472 Free PMC article.
-
Scintillating balloon-enabled fiber-optic system for radionuclide imaging of atherosclerotic plaques.J Nucl Med. 2015 May;56(5):771-7. doi: 10.2967/jnumed.114.153239. Epub 2015 Apr 9. J Nucl Med. 2015. PMID: 25858046 Free PMC article.
-
Complementary value of cardiac FDG PET and CT for the characterization of atherosclerotic disease.Radiographics. 2011 Sep-Oct;31(5):1255-69. doi: 10.1148/rg.315115028. Radiographics. 2011. PMID: 21918043 Review.
-
Targeted PET/CT imaging of vulnerable atherosclerotic plaques: microcalcification with sodium fluoride and inflammation with fluorodeoxyglucose.Curr Cardiol Rep. 2013 Jun;15(6):364. doi: 10.1007/s11886-013-0364-4. Curr Cardiol Rep. 2013. PMID: 23605466 Review.
Cited by
-
Single-Pixel MEMS Imaging Systems.Micromachines (Basel). 2020 Feb 20;11(2):219. doi: 10.3390/mi11020219. Micromachines (Basel). 2020. PMID: 32093324 Free PMC article. Review.
-
Non-Invasive Photoacoustic Imaging of In Vivo Mice with Erythrocyte Derived Optical Nanoparticles to Detect CAD/MI.Sci Rep. 2020 Apr 6;10(1):5983. doi: 10.1038/s41598-020-62868-1. Sci Rep. 2020. PMID: 32249814 Free PMC article.
-
Autofluorescence properties of balloon polymers used in medical applications.J Biomed Opt. 2020 Oct;25(10):106004. doi: 10.1117/1.JBO.25.10.106004. J Biomed Opt. 2020. PMID: 33084257 Free PMC article.
-
A Metabolic Intravascular Platform to Study FDG Uptake in Vascular Injury.Cardiovasc Eng Technol. 2020 Jun;11(3):328-336. doi: 10.1007/s13239-020-00457-z. Epub 2020 Jan 30. Cardiovasc Eng Technol. 2020. PMID: 32002814 Free PMC article.
-
In Vivo Translation of the CIRPI System: Revealing Molecular Pathology of Rabbit Aortic Atherosclerotic Plaques.J Nucl Med. 2019 Sep;60(9):1308-1316. doi: 10.2967/jnumed.118.222471. Epub 2019 Feb 8. J Nucl Med. 2019. PMID: 30737298 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
