

Abdominal Aortic Aneurysm: Evolving Controversies and Uncertainties
- PMID: 29896039
- PMCID: PMC5995687
- DOI: 10.1055/s-0038-1657771
Abdominal Aortic Aneurysm: Evolving Controversies and Uncertainties
Abstract
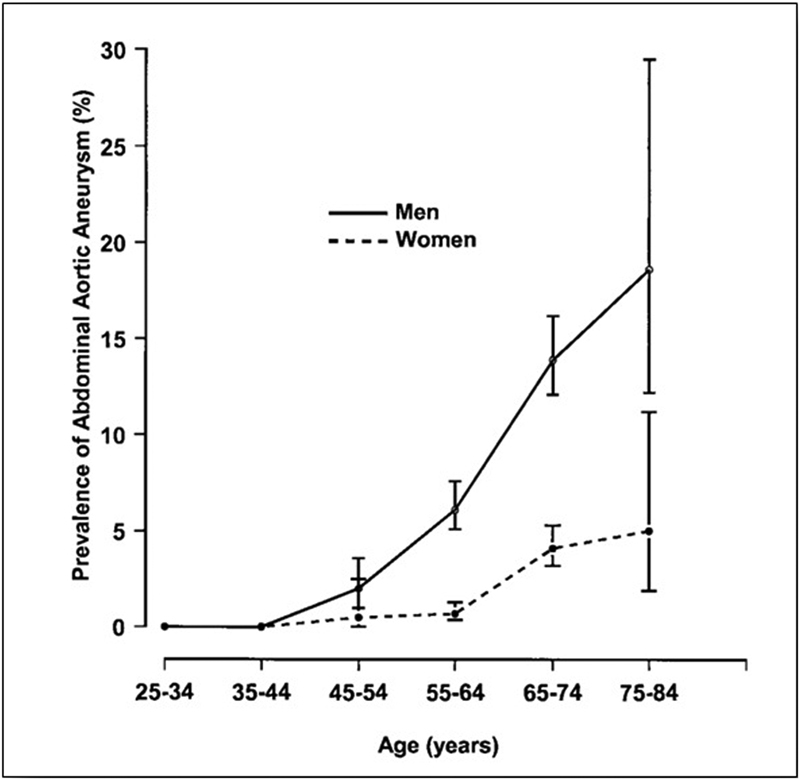
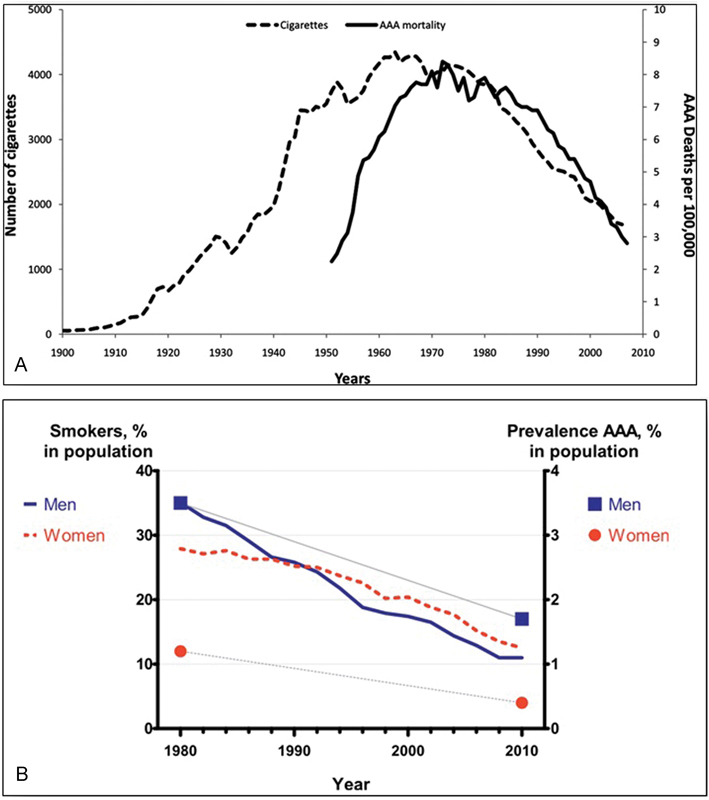
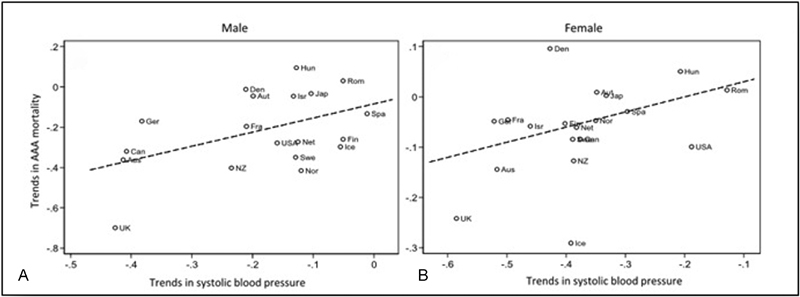
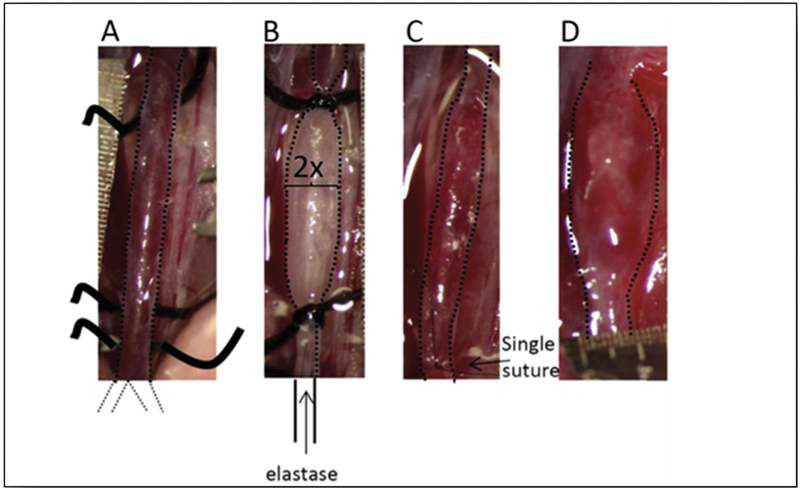
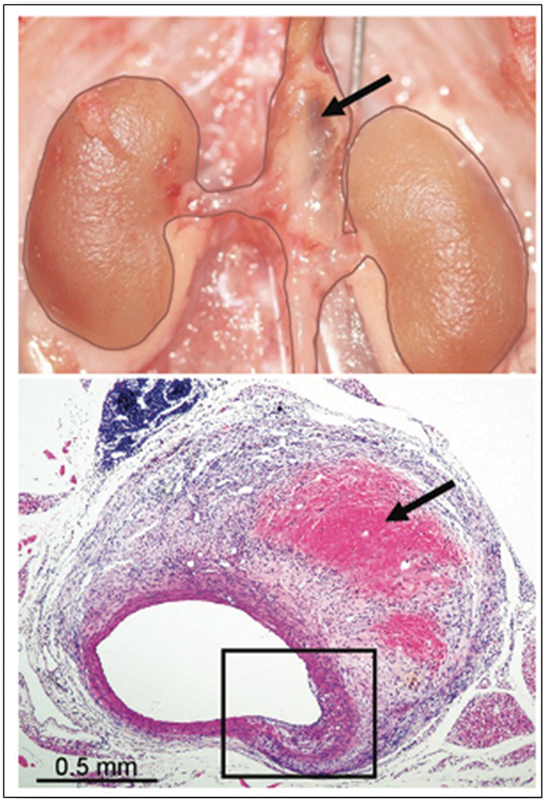
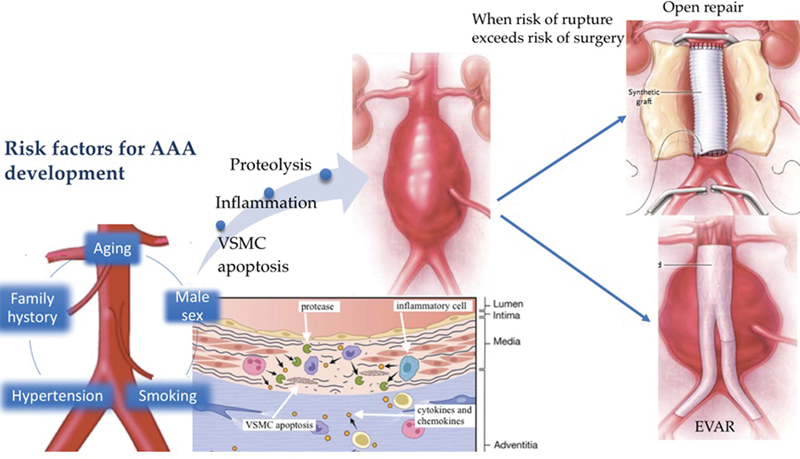
Abdominal aortic aneurysm (AAA) is defined as a permanent dilatation of the abdominal aorta that exceeds 3 cm. Most AAAs arise in the portion of abdominal aorta distal to the renal arteries and are defined as infrarenal. Most AAAs are totally asymptomatic until catastrophic rupture. The strongest predictor of AAA rupture is the diameter. Surgery is indicated to prevent rupture when the risk of rupture exceeds the risk of surgery. In this review, we aim to analyze this disease comprehensively, starting from an epidemiological perspective, exploring etiology and pathophysiology, and concluding with surgical controversies. We will pursue these goals by addressing eight specific questions regarding AAA: (1) Is the incidence of AAA increasing? (2) Are ultrasound screening programs for AAA effective? (3) What causes AAA: Genes versus environment? (4) Animal models: Are they really relevant? (5) What pathophysiology leads to AAA? (6) Indications for AAA surgery: Are surgeons over-eager to operate? (7) Elective AAA repair: Open or endovascular? (8) Emergency AAA repair: Open or endovascular?
Keywords: AAA; abdominal aortic aneurysm; animal models; endovascular aortic repair; indication for AAA surgery; risk factors; rupture AAA.
Conflict of interest statement
Figures
References
-
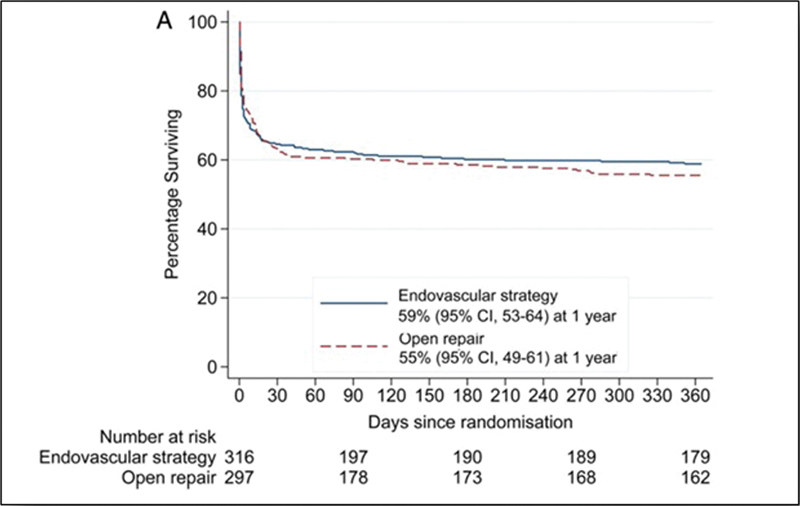
- van Beek S C, Conijn A P, Koelemay M J, Balm R. Editor's choice - endovascular aneurysm repair versus open repair for patients with a ruptured abdominal aortic aneurysm: a systematic review and meta-analysis of short-term survival. Eur J Vasc Endovasc Surg. 2014;47(06):593–602. - PubMed
-
- Sakalihasan N, Limet R, Defawe O D.Abdominal aortic aneurysm Lancet 2005365(9470):1577–1589. - PubMed
-
- Elefteriades J A, Rizzo J A. NY: Informa Healthcare USA; 2007. Epidemiology: incidence, prevalence, trends; pp. 89–97.
-
- Ingoldby C J, Wujanto R, Mitchell J E. Impact of vascular surgery on community mortality from ruptured aortic aneurysms. Br J Surg. 1986;73(07):551–553. - PubMed
-
- Johansson G, Swedenborg J. Ruptured abdominal aortic aneurysms: a study of incidence and mortality. Br J Surg. 1986;73(02):101–103. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
