

Outgrowing the Immaturity Myth: The Cost of Defending From Neonatal Infectious Disease
- PMID: 29896192
- PMCID: PMC5986917
- DOI: 10.3389/fimmu.2018.01077
Outgrowing the Immaturity Myth: The Cost of Defending From Neonatal Infectious Disease
Abstract
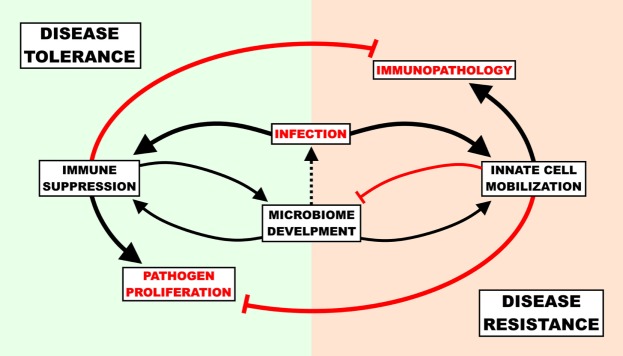
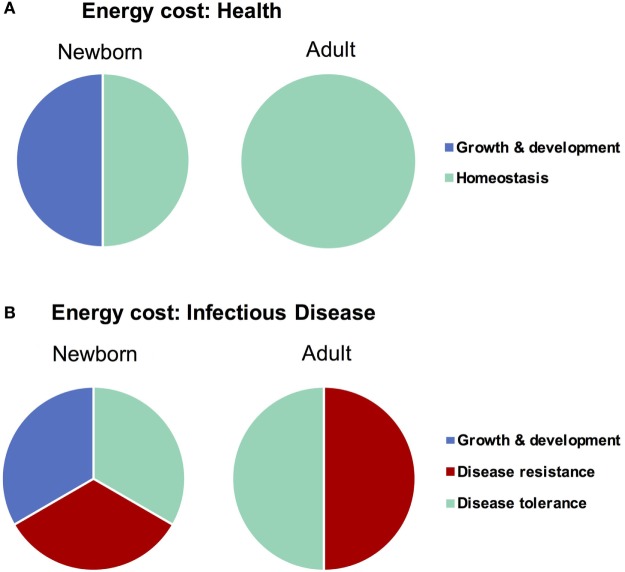
Newborns suffer high rates of mortality due to infectious disease-this has been generally regarded to be the result of an "immature" immune system with a diminished disease-fighting capacity. However, the immaturity dogma fails to explain (i) greater pro-inflammatory responses than adults in vivo and (ii) the ability of neonates to survive a significantly higher blood pathogen burden than of adults. To reconcile the apparent contradiction of clinical susceptibility to disease and the host immune response findings when contrasting newborn to adult, it will be essential to capture the entirety of available host-defense strategies at the newborn's disposal. Adults focus heavily on the disease resistance approach: pathogen reduction and elimination. Newborn hyperactive innate immunity, sensitivity to immunopathology, and the energetic requirements of growth and development (immune and energy costs), however, preclude them from having an adult-like resistance response. Instead, newborns also may avail themselves of disease tolerance (minimizing immunopathology without reducing pathogen load), as a disease tolerance approach provides a counterbalance to the dangers of a heightened innate immunity and has lower-associated immune costs. Further, disease tolerance allows for the establishment of a commensal bacterial community without mounting an unnecessarily dangerous immune resistance response. Since disease tolerance has its own associated costs (immune suppression leading to unchecked pathogen proliferation), it is the maintenance of homeostasis between disease tolerance and disease resistance that is critical to safe and effective defense against infections in early life. This paradigm is consistent with nearly all of the existing evidence.
Keywords: defense; infection; neonate; sepsis; tolerance.
Figures
Similar articles
-
Energy Demands of Early Life Drive a Disease Tolerant Phenotype and Dictate Outcome in Neonatal Bacterial Sepsis.Front Immunol. 2018 Aug 23;9:1918. doi: 10.3389/fimmu.2018.01918. eCollection 2018. Front Immunol. 2018. PMID: 30190719 Free PMC article. Review.
-
Newborn susceptibility to infection vs. disease depends on complex in vivo interactions of host and pathogen.Semin Immunopathol. 2017 Nov;39(6):615-625. doi: 10.1007/s00281-017-0651-z. Epub 2017 Nov 2. Semin Immunopathol. 2017. PMID: 29098373 Review.
-
Disease tolerance: concept and mechanisms.Curr Opin Immunol. 2018 Feb;50:88-93. doi: 10.1016/j.coi.2017.12.003. Epub 2017 Dec 15. Curr Opin Immunol. 2018. PMID: 29253642 Free PMC article. Review.
-
Disease Tolerance as an Inherent Component of Immunity.Annu Rev Immunol. 2019 Apr 26;37:405-437. doi: 10.1146/annurev-immunol-042718-041739. Epub 2019 Jan 23. Annu Rev Immunol. 2019. PMID: 30673535 Review.
-
Immunity by equilibrium.Nat Rev Immunol. 2016 Aug;16(8):524-32. doi: 10.1038/nri.2016.75. Epub 2016 Jul 11. Nat Rev Immunol. 2016. PMID: 27396446 Review.
Cited by
-
Composition of early life leukocyte populations in preterm infants with and without late-onset sepsis.PLoS One. 2022 Mar 2;17(3):e0264768. doi: 10.1371/journal.pone.0264768. eCollection 2022. PLoS One. 2022. PMID: 35235604 Free PMC article.
-
New Insights in Immunometabolism in Neonatal Monocytes and Macrophages in Health and Disease.Int J Mol Sci. 2023 Sep 16;24(18):14173. doi: 10.3390/ijms241814173. Int J Mol Sci. 2023. PMID: 37762476 Free PMC article. Review.
-
The composition of human vaginal microbiota transferred at birth affects offspring health in a mouse model.Nat Commun. 2021 Nov 1;12(1):6289. doi: 10.1038/s41467-021-26634-9. Nat Commun. 2021. PMID: 34725359 Free PMC article.
-
The Role of Iron in the Susceptibility of Neonatal Mice to Escherichia coli K1 Sepsis.J Infect Dis. 2019 Aug 30;220(7):1219-1229. doi: 10.1093/infdis/jiz282. J Infect Dis. 2019. PMID: 31136646 Free PMC article.
-
Advantages and Limitations of the Neonatal Immune System.Front Pediatr. 2020 Jan 28;8:5. doi: 10.3389/fped.2020.00005. eCollection 2020. Front Pediatr. 2020. PMID: 32047730 Free PMC article. Review.
References
-
- WHO. Causes of Child Mortality. Geneva: World Health Organization (WHO) (2016).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical