

Risk Factors of the Recurrences of Pancreatic Solid Pseudopapillary Tumors: A Systematic Review and Meta-analysis
- PMID: 29896274
- PMCID: PMC5995943
- DOI: 10.7150/jca.24491
Risk Factors of the Recurrences of Pancreatic Solid Pseudopapillary Tumors: A Systematic Review and Meta-analysis
Abstract
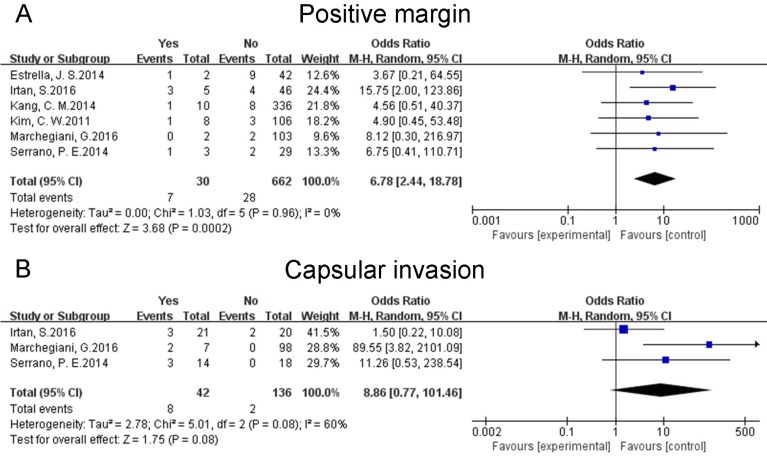
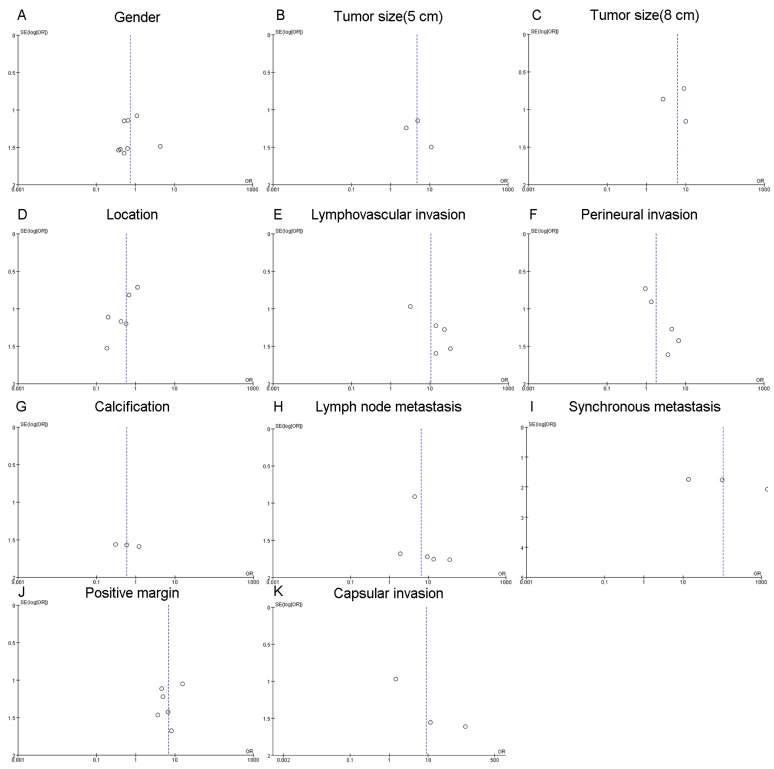
Background: Pancreatic solid pseudopapillary tumors (SPTs) are rare neoplasms with low-grade malignancy. The main treatment for them is surgical resection. However, some SPTs relapse after resection. The risk factors associated with the recurrences of resected SPTs remain controversial to date. We performed a systematic review and meta-analysis to identify the risk factors of the recurrences of pancreatic SPTs. Materials and Methods: We searched PubMed, EMBASE, and the Cochrane Library from their inception to December 2017. Studies that focused on the risk factors of postoperative relapses of pancreatic SPTs were enrolled. Combined ORs with 95% CIs were calculated to evaluate the effects of relevant factors investigated in eligible studies. Heterogeneity among combined results was assessed by Cochran's Q test and by the degree of inconsistency (I2). Statistical analyses were performed by Review Manager (version 5.3) using random effects models. Results: We included 10 studies, which enrolled 1091 patients. The pooled results suggested that patients with larger tumors (diameter > 5cm), lymphovascular invasion, lymph node metastasis, synchronous metastasis and positive margin were prone to suffer from the recurrences of SPTs. In addition, some factors like gender, location of tumors, perineural invasion, calcification and capsular invasion did not show any correlation with the relapses of resected SPTs. Conclusion: Factors including a larger tumor size (diameter > 5cm), lymphovascular invasion, lymph node metastasis, synchronous metastasis and positive margin may increase the risk of recurrences of resected pancreatic SPTs. All SPTs should be excised and patients with high-risk features should undergo a long-term follow-up.
Keywords: pancreatic solid pseudopapillary tumors; recurrence; risk factors.
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures




Similar articles
-
Natural history and malignant risk factors of solid pseudopapillary tumors of the pancreas.Postgrad Med. 2013 Mar;125(2):92-9. doi: 10.3810/pgm.2013.03.2634. Postgrad Med. 2013. PMID: 23816775
-
Solid pseudopapillary tumor of the pancreas suggesting malignant potential.Pancreas. 2006 Apr;32(3):276-80. doi: 10.1097/01.mpa.0000202956.41106.8a. Pancreas. 2006. PMID: 16628083
-
Small (<or=3 cm) solid pseudopapillary tumors of the pancreas at multiphasic multidetector CT.Radiology. 2010 Oct;257(1):97-106. doi: 10.1148/radiol.10092089. Epub 2010 Jul 27. Radiology. 2010. PMID: 20663966
-
Solid pseudopapillary tumor of the pancreas: A systematic review of clinical, surgical and oncological characteristics of 1384 patients underwent pancreatic surgery.Hepatobiliary Pancreat Dis Int. 2024 Aug;23(4):331-338. doi: 10.1016/j.hbpd.2023.05.004. Epub 2023 May 14. Hepatobiliary Pancreat Dis Int. 2024. PMID: 37236826
-
Risk of second primary tumors in GIST survivors: A systematic review and meta-analysis.Surg Oncol. 2019 Jun;29:64-70. doi: 10.1016/j.suronc.2019.03.001. Epub 2019 Mar 6. Surg Oncol. 2019. PMID: 31196495
Cited by
-
Solid-pseudopapillary Neoplasms of the Pancreas is still an Enigma: a Clinicopathological Review.Pathol Oncol Res. 2020 Apr;26(2):641-649. doi: 10.1007/s12253-019-00671-8. Epub 2019 Jun 17. Pathol Oncol Res. 2020. PMID: 31209654 Free PMC article. Review.
-
Development of a nomogram for predicting the high-risk groups of solid-pseudopapillary neoplasms of the pancreas.Front Oncol. 2024 Mar 15;13:1297497. doi: 10.3389/fonc.2023.1297497. eCollection 2023. Front Oncol. 2024. PMID: 38560421 Free PMC article.
-
The Sex Features of Patients With Solid Pseudopapillary Neoplasms of the Pancreas: A Retrospective Study.Front Oncol. 2022 Feb 18;12:844182. doi: 10.3389/fonc.2022.844182. eCollection 2022. Front Oncol. 2022. PMID: 35252013 Free PMC article.
-
Atypical solid pseudopapillary tumor of the pancreas in a 14-year-old.Clin Case Rep. 2021 Feb 2;9(3):1716-1720. doi: 10.1002/ccr3.3893. eCollection 2021 Mar. Clin Case Rep. 2021. PMID: 33768921 Free PMC article.
-
Clinicopathological factors associated with recurrence in patients undergoing resection of pancreatic solid pseudopapillary neoplasm.Discov Oncol. 2021 Nov 22;12(1):53. doi: 10.1007/s12672-021-00451-4. Discov Oncol. 2021. PMID: 35201506 Free PMC article.
References
-
- Frantz VK. Tumors of the pancreas. Atlas of tumor pathology Washington, DC: Armed forces Institute of Pathology; 1959. pp. 32–3.
-
- Kloppel G, Heitz PU, Capella C, Solcia E. Pathology and nomenclature of human gastrointestinal neuroendocrine (carcinoid) tumors and related lesions. World journal of surgery. 1996;20:132–41. - PubMed
-
- Yu P, Cheng X, Du Y, Yang L, Xu Z, Yin W. et al. Solid Pseudopapillary Neoplasms of the Pancreas: a 19-Year Multicenter Experience in China. J Gastrointest Surg. 2015;19:1433–40. - PubMed
-
- Galmiche L, Sarnacki S, Verkarre V, Boizet B, Duvillie B, Fabre M. et al. Transcription factors involved in pancreas development are expressed in paediatric solid pseudopapillary tumours. Histopathology. 2008;53:318–24. - PubMed
-
- Kosmahl M, Seada LS, Janig U, Harms D, Kloppel G. Solid-pseudopapillary tumor of the pancreas: its origin revisited. Virchows Archiv: an international journal of pathology. 2000;436:473–80. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
