

Mental stress as consequence and cause of vision loss: the dawn of psychosomatic ophthalmology for preventive and personalized medicine
- PMID: 29896314
- PMCID: PMC5972137
- DOI: 10.1007/s13167-018-0136-8
Mental stress as consequence and cause of vision loss: the dawn of psychosomatic ophthalmology for preventive and personalized medicine
Abstract
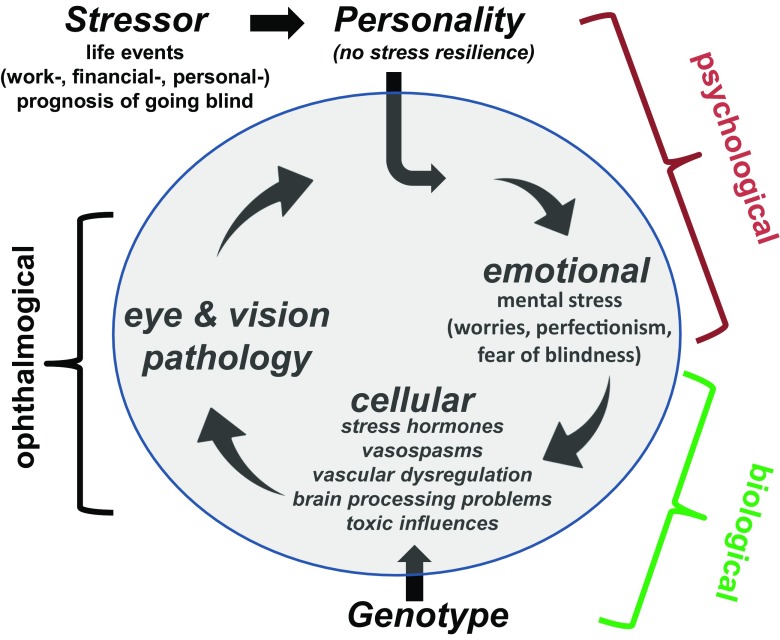
The loss of vision after damage to the retina, optic nerve, or brain has often grave consequences in everyday life such as problems with recognizing faces, reading, or mobility. Because vision loss is considered to be irreversible and often progressive, patients experience continuous mental stress due to worries, anxiety, or fear with secondary consequences such as depression and social isolation. While prolonged mental stress is clearly a consequence of vision loss, it may also aggravate the situation. In fact, continuous stress and elevated cortisol levels negatively impact the eye and brain due to autonomous nervous system (sympathetic) imbalance and vascular dysregulation; hence stress may also be one of the major causes of visual system diseases such as glaucoma and optic neuropathy. Although stress is a known risk factor, its causal role in the development or progression of certain visual system disorders is not widely appreciated. This review of the literature discusses the relationship of stress and ophthalmological diseases. We conclude that stress is both consequence and cause of vision loss. This creates a vicious cycle of a downward spiral, in which initial vision loss creates stress which further accelerates vision loss, creating even more stress and so forth. This new psychosomatic perspective has several implications for clinical practice. Firstly, stress reduction and relaxation techniques (e.g., meditation, autogenic training, stress management training, and psychotherapy to learn to cope) should be recommended not only as complementary to traditional treatments of vision loss but possibly as preventive means to reduce progression of vision loss. Secondly, doctors should try their best to inculcate positivity and optimism in their patients while giving them the information the patients are entitled to, especially regarding the important value of stress reduction. In this way, the vicious cycle could be interrupted. More clinical studies are now needed to confirm the causal role of stress in different low vision diseases to evaluate the efficacy of different anti-stress therapies for preventing progression and improving vision recovery and restoration in randomized trials as a foundation of psychosomatic ophthalmology.
Keywords: Low vision; Personalized medicine; Predictive; Preventive; Psychology; Psychosomatic medicine; Relaxation; Restoration; Stress.
Conflict of interest statement
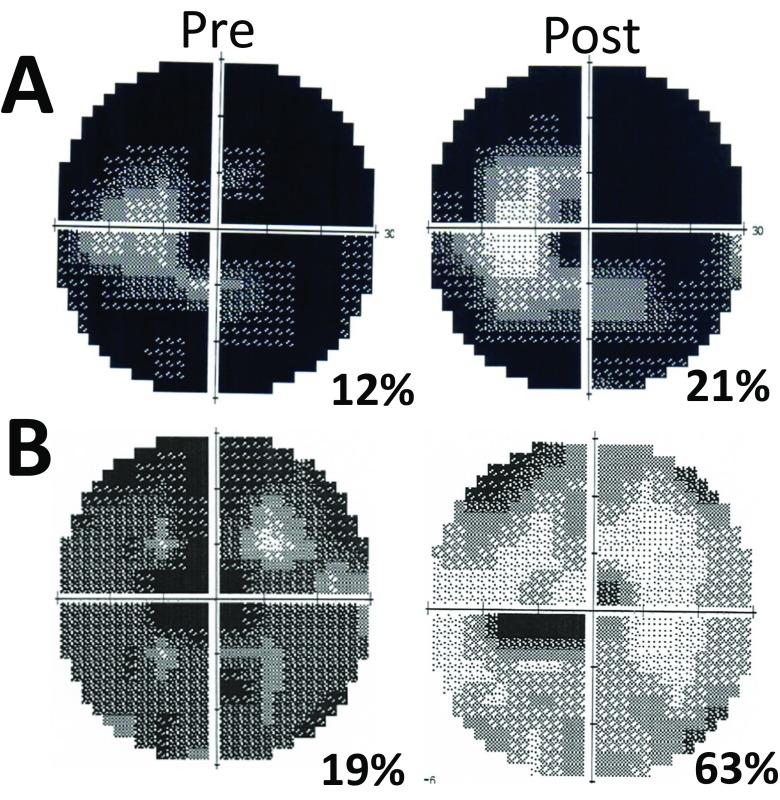
Compliance with ethical standardsB. Sabel is co-owner of a private medical practice (www.savir-center.com) where the two patients described in this paper were treated.For this type of study, formal consent is not required. We thank our patients for their consent to publish their case histories.
Figures
Similar articles
-
Personality and stress influence vision restoration and recovery in glaucoma and optic neuropathy following alternating current stimulation: implications for personalized neuromodulation and rehabilitation.EPMA J. 2020 Apr 13;11(2):177-196. doi: 10.1007/s13167-020-00204-3. eCollection 2020 Jun. EPMA J. 2020. PMID: 32547650 Free PMC article.
-
Is Mental Stress the Primary Cause of Glaucoma?Klin Monbl Augenheilkd. 2021 Feb;238(2):132-145. doi: 10.1055/a-1303-8025. Epub 2021 Feb 12. Klin Monbl Augenheilkd. 2021. PMID: 33578436 English, German.
-
Residual vision activation and the brain-eye-vascular triad: Dysregulation, plasticity and restoration in low vision and blindness - a review.Restor Neurol Neurosci. 2018;36(6):767-791. doi: 10.3233/RNN-180880. Restor Neurol Neurosci. 2018. PMID: 30412515 Free PMC article. Review.
-
The effectiveness of mindfulness based programs in reducing stress experienced by nurses in adult hospital settings: a systematic review of quantitative evidence protocol.JBI Database System Rev Implement Rep. 2015 Oct;13(10):21-9. doi: 10.11124/jbisrir-2015-2380. JBI Database System Rev Implement Rep. 2015. PMID: 26571279
-
[Are Visual Field Defects Reversible? - Visual Rehabilitation with Brains].Klin Monbl Augenheilkd. 2017 Feb;234(2):194-204. doi: 10.1055/s-0042-104588. Epub 2016 Aug 9. Klin Monbl Augenheilkd. 2017. PMID: 27504612 Review. German.
Cited by
-
Clinical Landscape of Central Serous Chorioretinopathy in Germany: Retina.net CSC Registry Report Number 1.Ophthalmologica. 2024;247(2):95-106. doi: 10.1159/000535930. Epub 2024 Feb 16. Ophthalmologica. 2024. PMID: 38368867 Free PMC article.
-
Common mental illness in people with sensory impairment: results from the 2014 adult psychiatric morbidity survey.BJPsych Open. 2019 Nov 5;5(6):e94. doi: 10.1192/bjo.2019.81. BJPsych Open. 2019. PMID: 31685070 Free PMC article.
-
Relationship between ocular biometry and severity of primary angle-closure glaucoma: relevance for predictive, preventive, and personalized medicine.EPMA J. 2019 Jun 11;10(3):261-271. doi: 10.1007/s13167-019-00174-1. eCollection 2019 Sep. EPMA J. 2019. PMID: 31462943 Free PMC article.
-
Associations between the red blood cell distribution width and primary angle-closure glaucoma: a potential for disease prediction.EPMA J. 2019 Apr 5;10(2):185-193. doi: 10.1007/s13167-019-00166-1. eCollection 2019 Jun. EPMA J. 2019. PMID: 31258822 Free PMC article.
-
A Glimpse into the mysteries of glaucoma: From theories to clinics.Oman J Ophthalmol. 2019 Jan-Apr;12(1):1-3. doi: 10.4103/ojo.OJO_91_2018. Oman J Ophthalmol. 2019. PMID: 30787526 Free PMC article. No abstract available.
References
-
- WHO. Visual impairment and blindness. 2014.
-
- Sabel BA, Fedorov A, Henrich-Noack P, Gall C. Vision restoration after brain damage: the “residual vision activation theory”. Prog Brain Res. 2010;192:199–262. - PubMed
-
- Kasten E, Wüst S, Behrens-Baumann W, et al. Computer-based training for the treatment of partial blindness. Nat Med. 1998;4:1083–1087. - PubMed
-
- Sabel BA, Gudlin J. Vision restoration training for Glaucoma. A randomized clinical trial. JAMA Ophthalmology. 2014;132:381–389. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
