

Urinary Neutrophil Gelatinase-Associated Lipocalin Is Excellent Predictor of Acute Kidney Injury in Septic Elderly Patients
- PMID: 29896409
- PMCID: PMC5963341
- DOI: 10.14336/AD.2017.0307
Urinary Neutrophil Gelatinase-Associated Lipocalin Is Excellent Predictor of Acute Kidney Injury in Septic Elderly Patients
Abstract
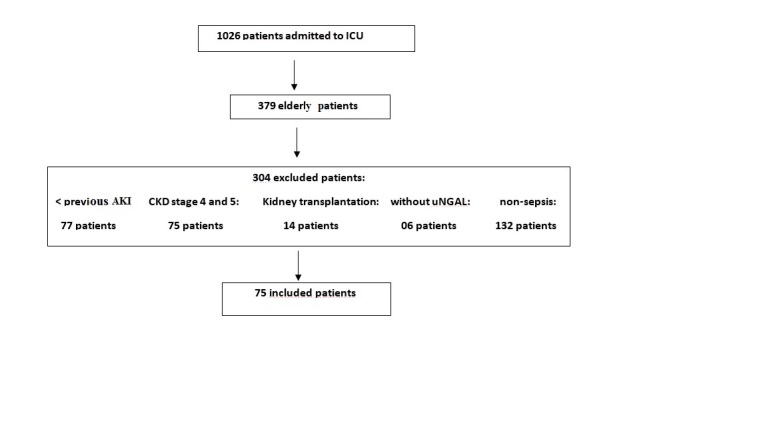
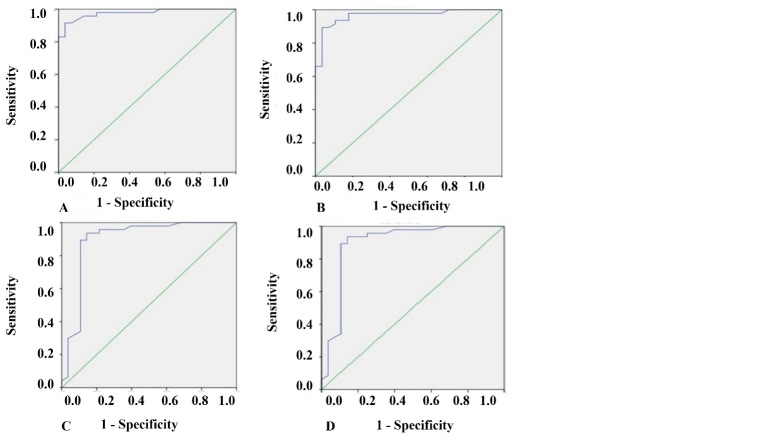
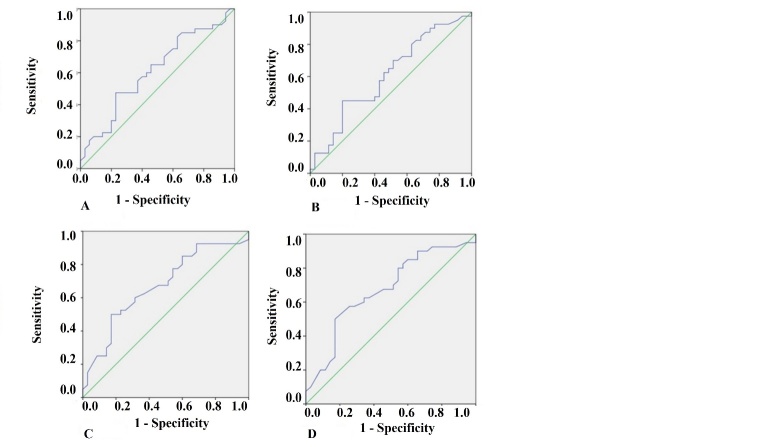
Elderly is the main age group affected by acute kidney injury (AKI). There are no studies that investigated the predictive properties of urinary (u) NGAL as an AKI marker in septic elderly population. This study aimed to evaluate the efficacy of uNGAL as predictor of AKI diagnosis and prognosis in elderly septic patients admitted to ICUs. We prospectively studied elderly patients with sepsis admitted to ICUs from October 2014 to November 2015. Assessment of renal function was performed daily by serum creatinine and urine output. The level of uNGAL was performed within the first 48 hours of the diagnosis of sepsis (NGAL1) and between 48 and 96 hours (NGAL2). The results were presented using descriptive statistics and area under the receiver operating characteristic curve (AUC-ROC) and p value was 5%. Seventy-five patients were included, 47 (62.7%) developed AKI. At logistic regression, chronic kidney disease and low mean blood pressure at admission were identified as factors associated with AKI (OR=0.05, CI=0.01-0.60, p=0.045 and OR=0.81, CI=0,13-0.47; p=0.047). The uNGAL was excellent predictor of AKI diagnosis (AUC-ROC >0.95, and sensitivity and specificity>0.89), anticipating the AKI diagnosis in 2.1±0.3 days. Factors associated with mortality in the logistic regression were presence of AKI (OR=2.14, CI=1.42-3.98, p=0.04), chronic obstructive pulmonary disease (OR = 9.37, CI =1.79-49.1, p=0.008) and vasoactive drugs (OR=2.06, CI=0.98-1.02, p=0.04). The accuracy of NGALu 1 and 2 as predictors of death was intermediate, with AUC-ROC of 0.61 and 0.62; sensitivity between 0.65 and 0.77 and specificity lower than 0.6. The uNGAL was excellent predictor of AKI in septic elderly patients in ICUs and can anticipate the diagnosis of AKI in 2.1 days.
Keywords: NGAL; acute kidney injury; biomarker; elderly.
Figures
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR (2001). Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med, 9: 1303-10. - PubMed
-
- Zarjou A, Agarwal A (2011). Sepsis and acute kidney injury. J Am Soc Nephrol JASN, 22(6): 999-1006. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous