

Are traditional scoring systems for severity stratification of acute pancreatitis sufficient?
- PMID: 29896571
- PMCID: PMC5981140
- DOI: 10.14701/ahbps.2018.22.2.105
Are traditional scoring systems for severity stratification of acute pancreatitis sufficient?
Abstract
Backgrounds/aims: Ranson's score (RS) and Glasgow score (GS) have been utilized to stratify the severity of acute pancreatitis (AP). The aim of this study was to validate RS and GS for stratifying the severity of acute pancreatitis and audit our experience of managing AP.
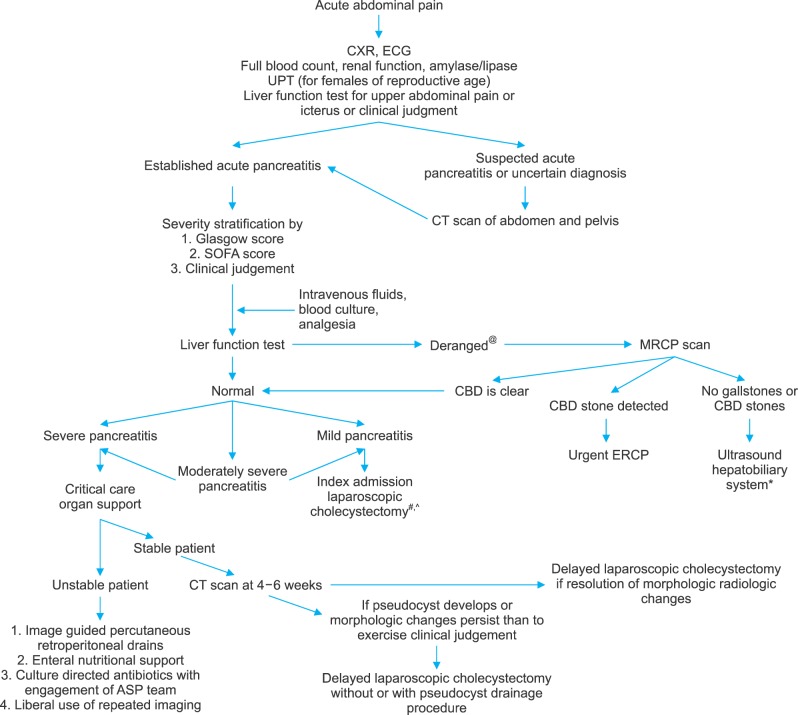
Methods: We conducted a retrospective review of patients treated for AP from July 2009 to September 2016. Final severity was determined using the revised Atlanta classification. Mortality and complications were analyzed.
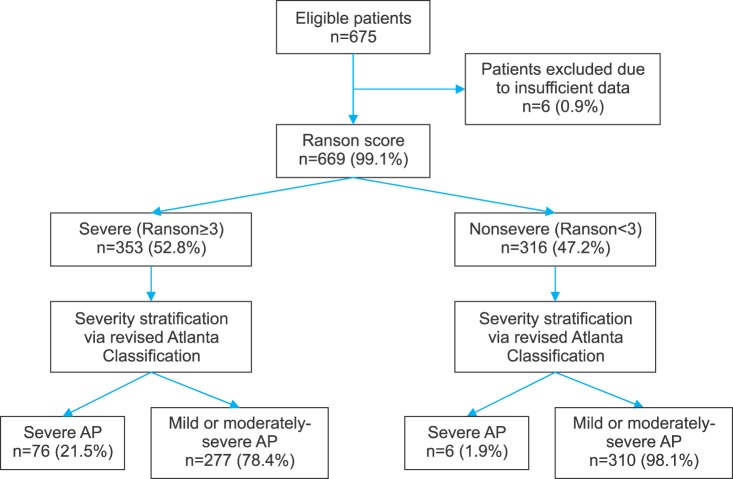
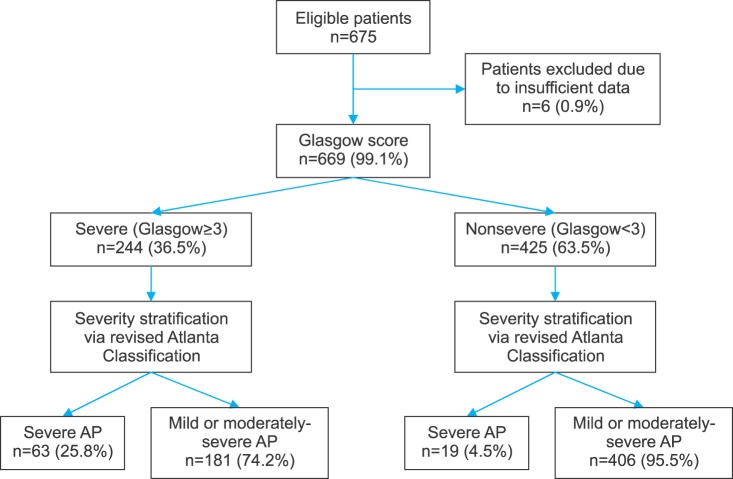
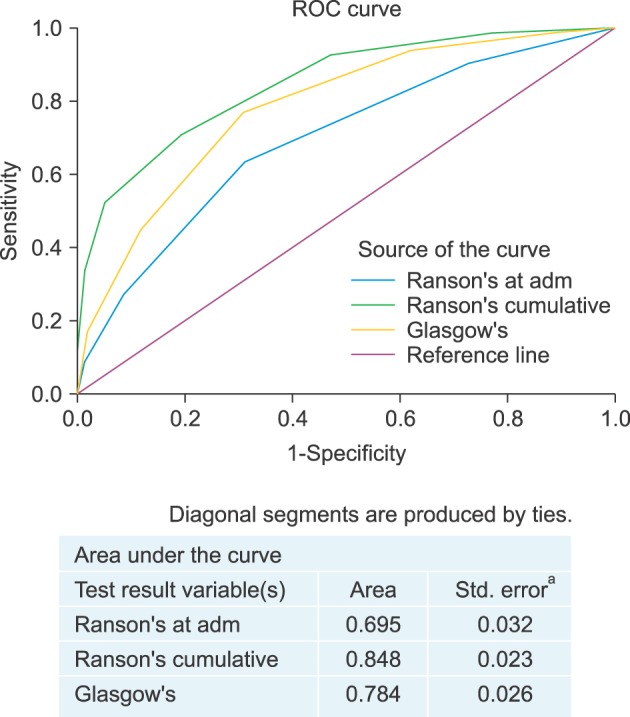
Results: From July 2009 to September 2016, a total of 675 patients with a diagnosis of AP were admitted at the hospital. Of them, 669 patients who had sufficient data were analyzed. Their average age±SD was 58.7±17.4 years (range, 21-98 years). There was a male preponderance (n=393, 53.8%). A total of 82 (12.3%) patients had eventual severe pancreatitis. RS demonstrated a sensitivity of 92.7% and a specificity of 52.8% with a positive predictive value (PPV) of 21.5% and a negative predictive value (NPV) of 98.1%. GS demonstrated a sensitivity of 76.8% and a specificity of 69.2% with a PPV of 25.8% and a NPV of 95.5%. For severity prediction, areas under the curve (AUCs) for RS and GS were 0.848 (95% CI: 0.819-0.875) and 0.784 (95% CI: 0.750-0.814), respectively (p=0.003). Twelve (1.6%) patients died in the hospital.
Conclusions: RS has higher sensitivity, NPV and AUC for predicting severity of AP than GS.
Keywords: Glasgow score; Ranson score; Scoring; Severe acute pancreatitis.
Figures
References
-
- Clancy TE, Benoit EP, Ashley SW. Current management of acute pancreatitis. J Gastrointest Surg. 2005;9:440–452. - PubMed
-
- Tenner S, Baillie J, DeWitt J, Vege SS American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis. Am J Gastroenterol. 2013;108:1400–1415. 1416. - PubMed
-
- Banks PA, Freeman ML Practice Parameters Committee of the American College of Gastroenterology. Practice guidelines in acute pancreatitis. Am J Gastroenterol. 2006;101:2379–2400. - PubMed
-
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62:102–111. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources