

Management of very late peritoneal metastasis of hepatocellular carcinoma 10 years after liver transplantation: Lessons from two cases
- PMID: 29896574
- PMCID: PMC5981143
- DOI: 10.14701/ahbps.2018.22.2.136
Management of very late peritoneal metastasis of hepatocellular carcinoma 10 years after liver transplantation: Lessons from two cases
Abstract
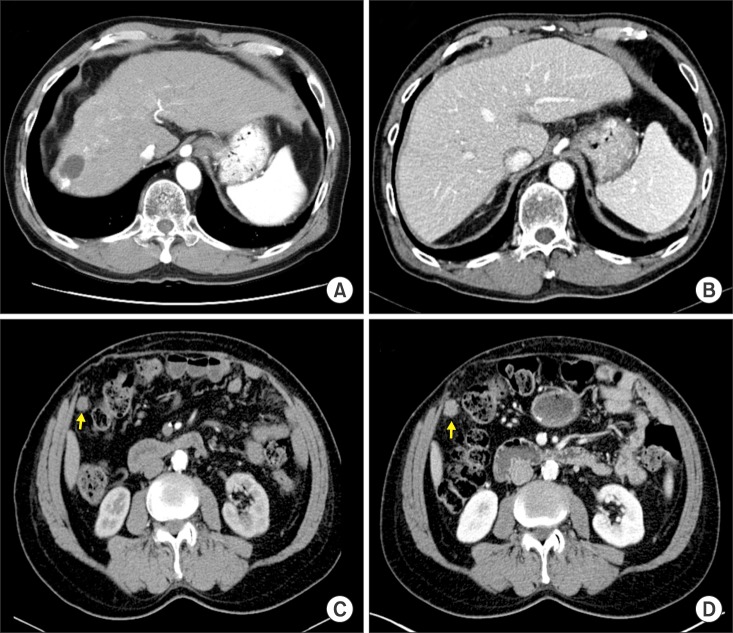
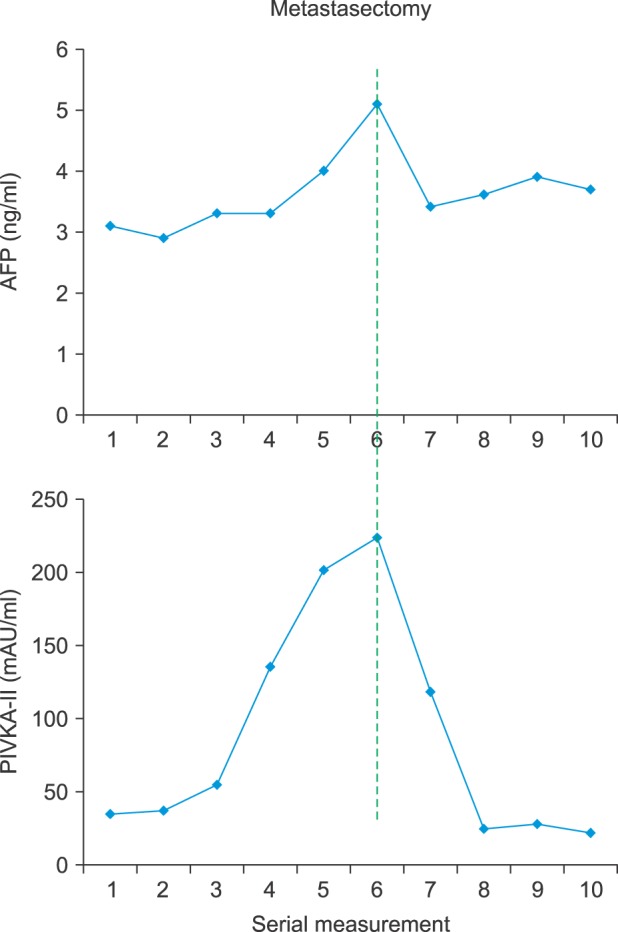
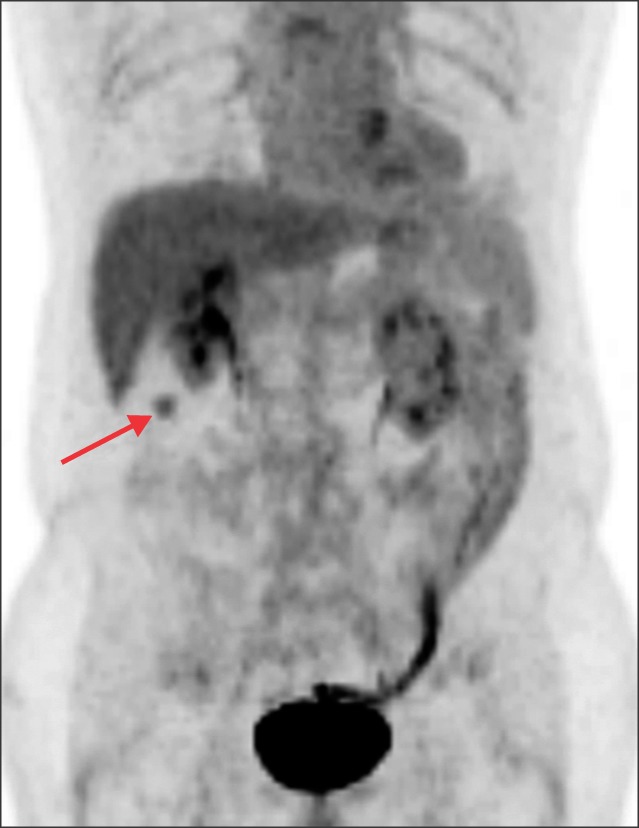
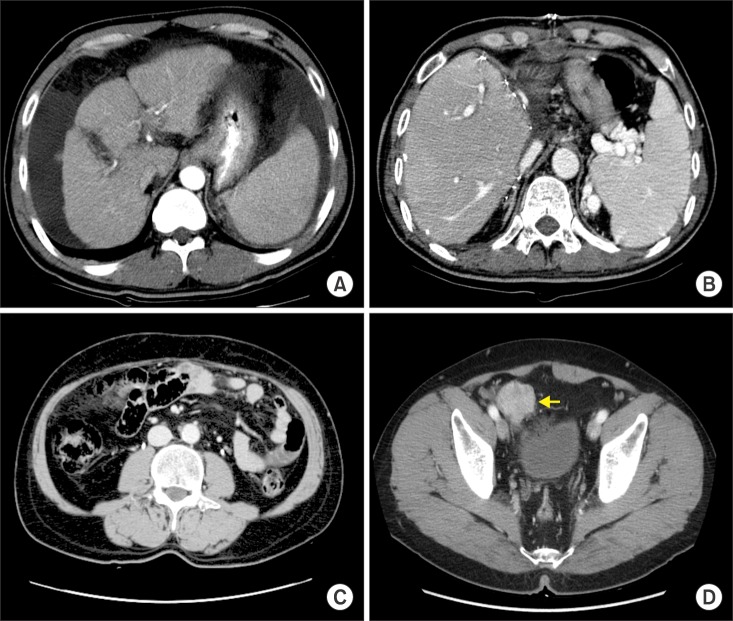
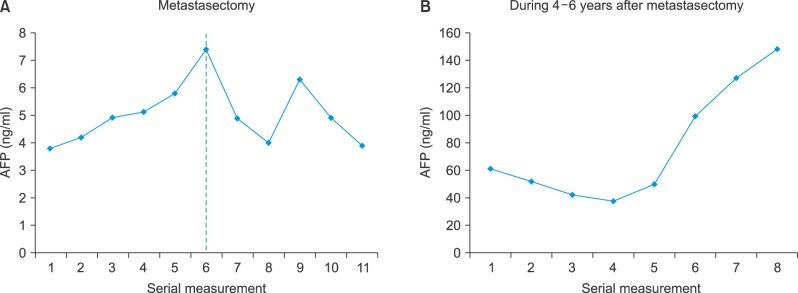
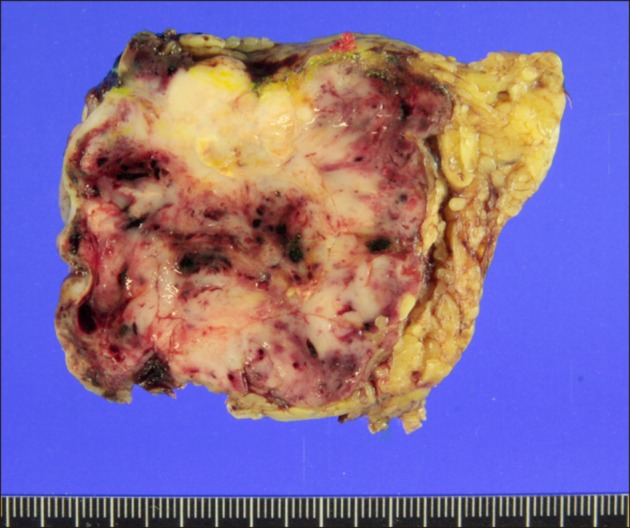
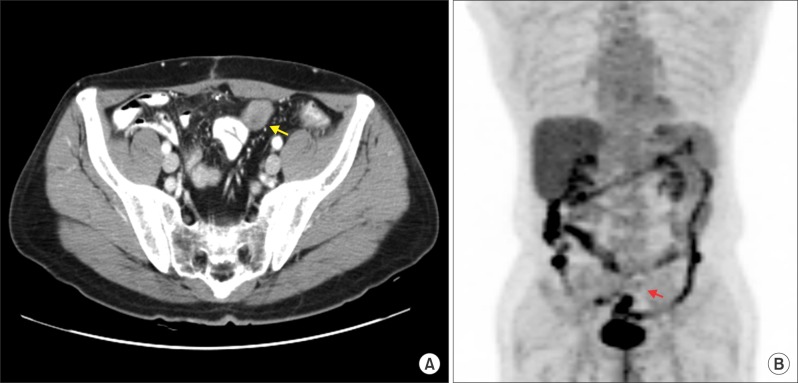
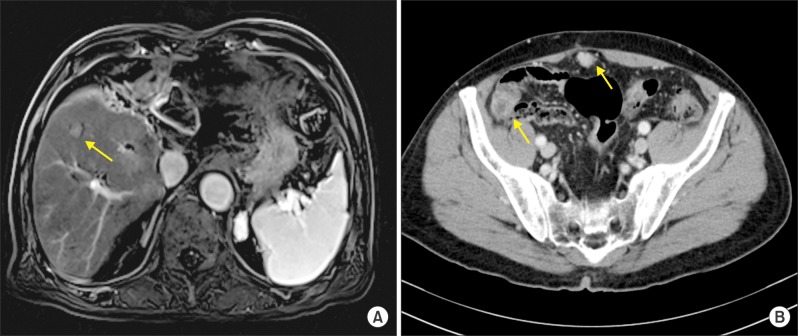
Recurrence of hepatocellular carcinoma (HCC) 10 years after liver transplantation (LT) is very rare. Here, we present two cases of peritoneal metastasis of HCC that occurred 10 and 12 years after LT. A 77-year-old male who had undergone deceased-donor LT 10 years earlier showed slow progressive elevation of tumor marker levels over 6 months. Close observation with frequent imaging studies and monthly tumor marker analyses revealed a solitary peritoneal seeding mass. Imaging studies revealed that the mass was highly likely to be metastatic HCC. After excision of the mass, all tumor markers returned to the normal range. Over past 10 months, the patient has received everolimus monotherapy and half-dose sorafenib, and has shown no evidence of HCC recurrence. In the second case, marginally elevated tumor marker levels were detected in a 65-year-old male who had undergone living-donor LT 12 years earlier. After observation for 3 months, follow-up studies revealed a peritoneal seeding mass. Thorough imaging studies revealed that the mass was highly likely to be metastatic HCC. Two mass lesions were excised, and the patient was administered low-dose calcineruin inhibitor, sirolimus, and full-dose sorafenib. Subsequently, the tumor marker levels increased again and growth of new peritoneal seeding nodules was observed; therefore, sorafenib was stopped after 2 years of administration. During 6 years since HCC recurrence diagnosis, the patient has experienced slowly growing tumors, but has been doing well. For very late peritoneal metastasis of HCC, the therapeutic modalities include surgical resection if possible, everolimus monotherapy, and long-term use of sorafenib.
Keywords: Hepatocellular carcinoma; Metastasis; Recurrence; Resection; Sorafenib.
Figures

References
-
- Lee SG, Hwang S, Moon DB, Ahn CS, Kim KH, Sung KB, et al. Expanded indication criteria of living donor liver transplantation for hepatocellular carcinoma at one large-volume center. Liver Transpl. 2008;14:935–945. - PubMed
-
- Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–699. - PubMed
-
- Hwang S, Lee SG, Joh JW, Suh KS, Kim DG. Liver transplantation for adult patients with hepatocellular carcinoma in Korea: comparison between cadaveric donor and living donor liver transplantations. Liver Transpl. 2005;11:1265–1272. - PubMed
-
- Yao FY, Ferrell L, Bass NM, Watson JJ, Bacchetti P, Venook A, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001;33:1394–1403. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous