

Strong Relation Between Muscle Mass Determined by D3-creatine Dilution, Physical Performance, and Incidence of Falls and Mobility Limitations in a Prospective Cohort of Older Men
- PMID: 29897420
- PMCID: PMC6521914
- DOI: 10.1093/gerona/gly129
Strong Relation Between Muscle Mass Determined by D3-creatine Dilution, Physical Performance, and Incidence of Falls and Mobility Limitations in a Prospective Cohort of Older Men
Abstract
Background: Direct assessment of skeletal muscle mass in older adults is clinically challenging. Relationships between lean mass and late-life outcomes have been inconsistent. The D3-creatine dilution method provides a direct assessment of muscle mass.
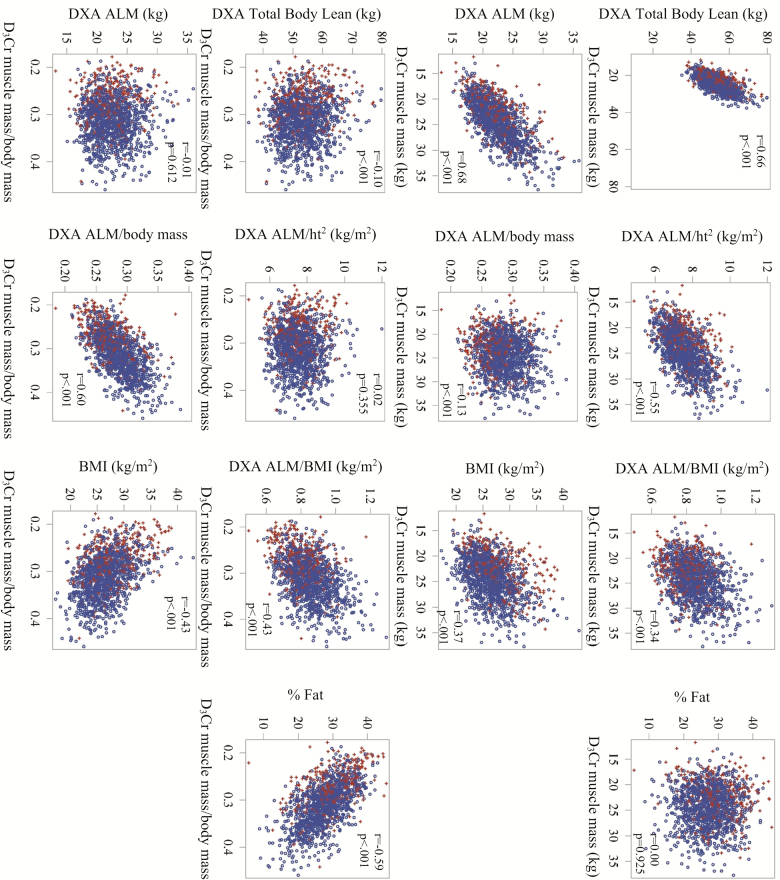
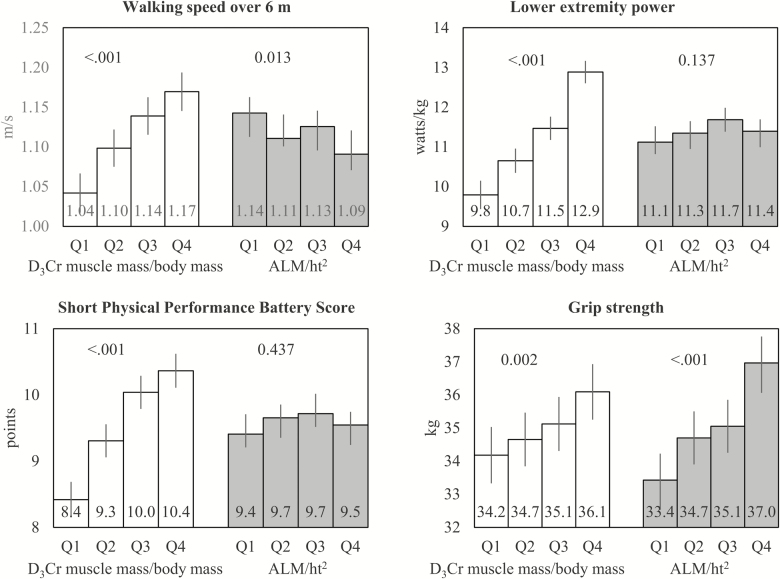
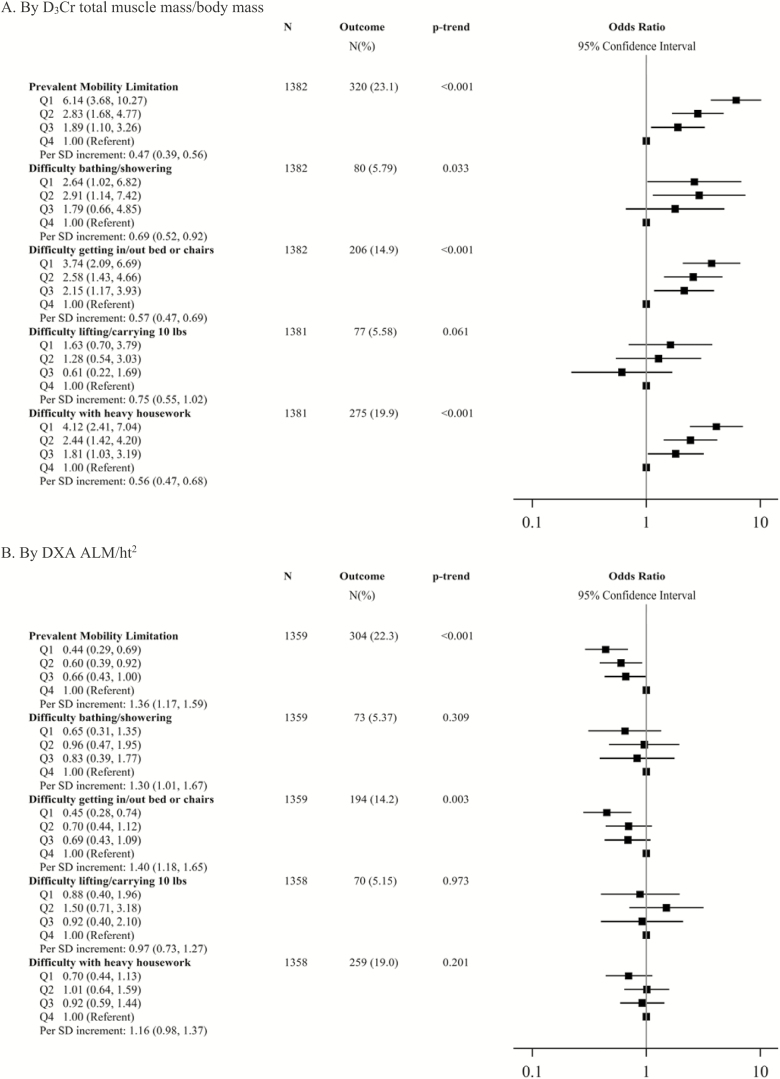
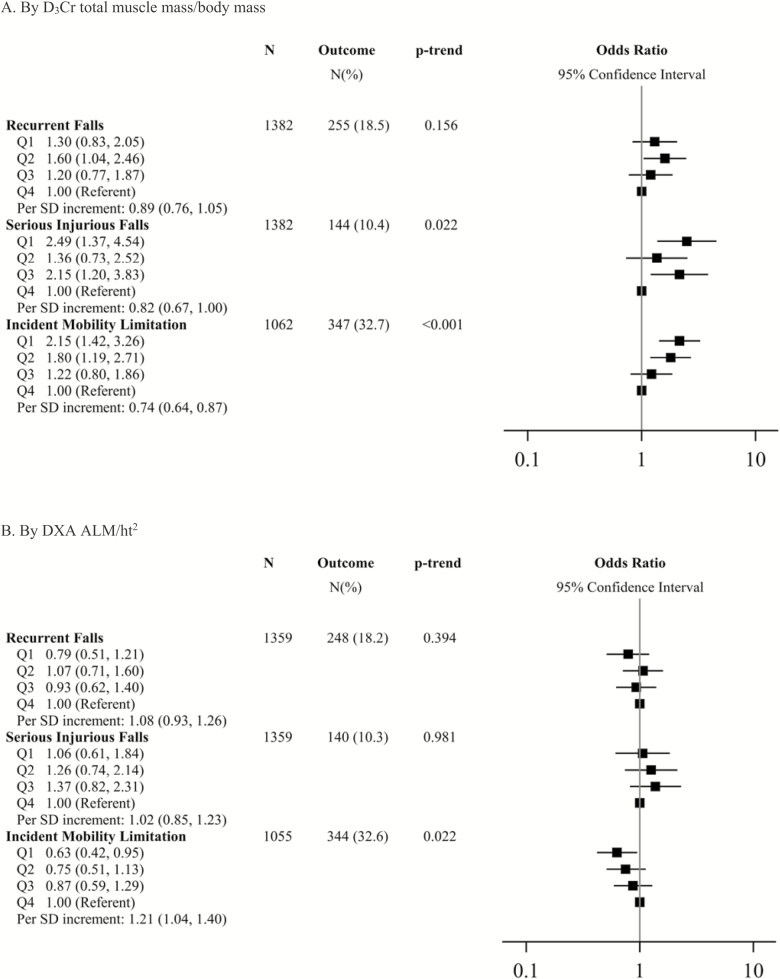
Methods: Muscle mass was assessed by D3-creatine (D3Cr) dilution in 1,382 men (mean age, 84.2 years). Participants completed the Short Physical Performance Battery (SPPB); usual walking speed (6 m); and dual x-ray absorptiometry (DXA) lean mass. Men self-reported mobility limitations (difficulty walking 2-3 blocks or climbing 10 steps); recurrent falls (2+); and serious injurious falls in the subsequent year. Across quartiles of D3Cr muscle mass/body mass, multivariate linear models calculated means for SPPB and gait speed; multivariate logistic models calculated odds ratios for incident mobility limitations or falls.
Results: Compared to men in the highest quartile, those in the lowest quartile of D3Cr muscle mass/body mass had slower gait speed (Q1: 1.04 vs Q4: 1.17 m/s); lower SPPB (Q1: 8.4 vs Q4: 10.4 points); greater likelihood of incident serious injurious falls (odds ratio [OR] Q1 vs Q4: 2.49, 95% confidence interval [CI]: 1.37, 4.54); prevalent mobility limitation (OR Q1 vs Q4,: 6.1, 95% CI: 3.7, 10.3) and incident mobility limitation (OR Q1 vs Q4: 2.15 95% CI: 1.42, 3.26); p for trend < .001 for all. Results for incident recurrent falls were in the similar direction (p = .156). DXA lean mass had weaker associations with the outcomes.
Conclusions: Unlike DXA lean mass, low D3Cr muscle mass/body mass is strongly related to physical performance, mobility, and incident injurious falls in older men.
Keywords: Falls; Functional performance; Muscle; Sarcopenia.
© The Author(s) 2018. Published by Oxford University Press on behalf of The Gerontological Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
D3-Creatine Dilution to Assess Muscle Mass.J Gerontol A Biol Sci Med Sci. 2019 May 16;74(6):842-843. doi: 10.1093/gerona/gly180. J Gerontol A Biol Sci Med Sci. 2019. PMID: 30215688 No abstract available.
References
-
- Cawthon PM, Fox KM, Gandra SR, et al. ; Health, Aging and Body Composition Study Do muscle mass, muscle density, strength, and physical function similarly influence risk of hospitalization in older adults?J Am Geriatr Soc. 2009;57:1411–1419. doi: 10.1111/j.1532-5415.2009.02366.x - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
