

Transdiagnostic Risk Calculator for the Automatic Detection of Individuals at Risk and the Prediction of Psychosis: Second Replication in an Independent National Health Service Trust
- PMID: 29897527
- PMCID: PMC6483570
- DOI: 10.1093/schbul/sby070
Transdiagnostic Risk Calculator for the Automatic Detection of Individuals at Risk and the Prediction of Psychosis: Second Replication in an Independent National Health Service Trust
Abstract
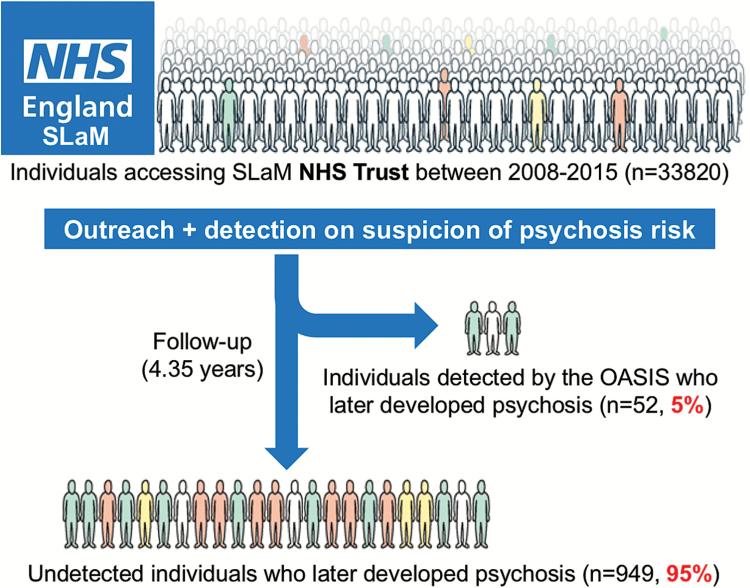
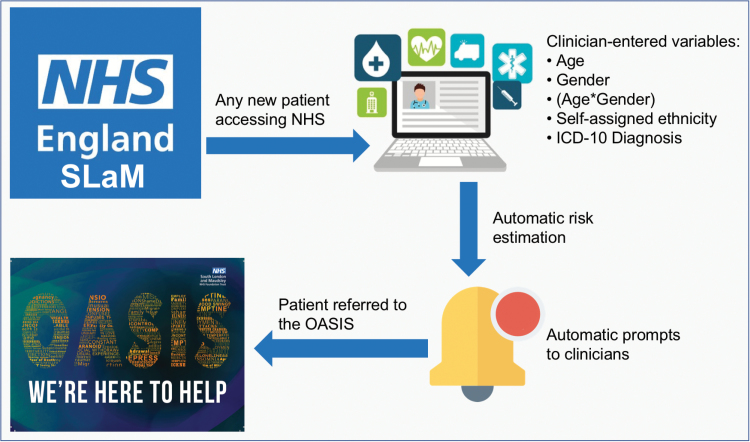
Background: The benefits of indicated primary prevention among individuals at Clinical High Risk for Psychosis (CHR-P) are limited by the difficulty in detecting these individuals. To overcome this problem, a transdiagnostic, clinically based, individualized risk calculator has recently been developed and subjected to a first external validation in 2 different catchment areas of the South London and Maudsley (SLaM) NHS Trust.
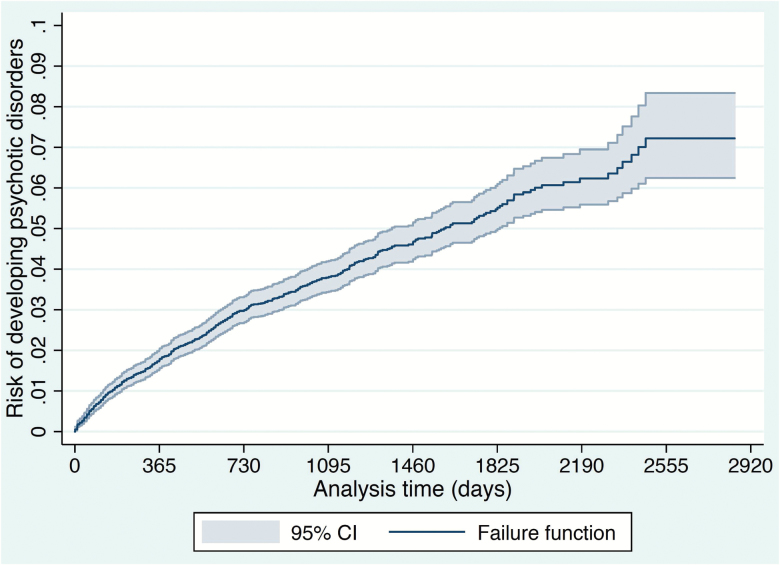
Methods: Second external validation of real world, real-time electronic clinical register-based cohort study. All individuals who received a first ICD-10 index diagnosis of nonorganic and nonpsychotic mental disorder within the Camden and Islington (C&I) NHS Trust between 2009 and 2016 were included. The model previously validated included age, gender, ethnicity, age by gender, and ICD-10 index diagnosis to predict the development of any ICD-10 nonorganic psychosis. The model's performance was measured using Harrell's C-index.
Results: This study included a total of 13702 patients with an average age of 40 (range 16-99), 52% were female, and most were of white ethnicity (64%). There were no CHR-P or child/adolescent services in the C&I Trust. The C&I and SLaM Trust samples also differed significantly in terms of age, gender, ethnicity, and distribution of index diagnosis. Despite these significant differences, the original model retained an acceptable predictive performance (Harrell's C of 0.73), which is comparable to that of CHR-P tools currently recommended for clinical use.
Conclusions: This risk calculator may pragmatically support an improved transdiagnostic detection of at-risk individuals and psychosis prediction even in NHS Trusts in the United Kingdom where CHR-P services are not provided.
Keywords: psychosis; risk calculator; schizophrenia; transdiagnostic; validation.
© The Author(s) 2018. Published by Oxford University Press on behalf of the Maryland Psychiatric Research Center.
Figures
Similar articles
-
Development and Validation of a Clinically Based Risk Calculator for the Transdiagnostic Prediction of Psychosis.JAMA Psychiatry. 2017 May 1;74(5):493-500. doi: 10.1001/jamapsychiatry.2017.0284. JAMA Psychiatry. 2017. PMID: 28355424 Free PMC article.
-
Transdiagnostic Individualized Clinically Based Risk Calculator for the Detection of Individuals at Risk and the Prediction of Psychosis: Model Refinement Including Nonlinear Effects of Age.Front Psychiatry. 2019 May 9;10:313. doi: 10.3389/fpsyt.2019.00313. eCollection 2019. Front Psychiatry. 2019. PMID: 31143134 Free PMC article.
-
Using Natural Language Processing on Electronic Health Records to Enhance Detection and Prediction of Psychosis Risk.Schizophr Bull. 2021 Mar 16;47(2):405-414. doi: 10.1093/schbul/sbaa126. Schizophr Bull. 2021. PMID: 33025017 Free PMC article.
-
Individualized Prediction of Transition to Psychosis in 1,676 Individuals at Clinical High Risk: Development and Validation of a Multivariable Prediction Model Based on Individual Patient Data Meta-Analysis.Front Psychiatry. 2019 May 21;10:345. doi: 10.3389/fpsyt.2019.00345. eCollection 2019. Front Psychiatry. 2019. PMID: 31178767 Free PMC article.
-
[Detection and early treatment of subjects at high risk of clinical psychosis: Definitions and recommendations].Encephale. 2017 May;43(3):292-297. doi: 10.1016/j.encep.2017.01.005. Epub 2017 Mar 25. Encephale. 2017. PMID: 28347521 Review. French.
Cited by
-
Transdiagnostic risk of mental disorders in offspring of affected parents: a meta-analysis of family high-risk and registry studies.World Psychiatry. 2023 Oct;22(3):433-448. doi: 10.1002/wps.21147. World Psychiatry. 2023. PMID: 37713573 Free PMC article.
-
Translating RDoC to Real-World Impact in Developmental Psychopathology: A Neurodevelopmental Framework for Application of Mental Health Risk Calculators.Dev Psychopathol. 2021 Dec;33(5):1665-1684. doi: 10.1017/s0954579421000651. Epub 2021 Dec 7. Dev Psychopathol. 2021. PMID: 35095215 Free PMC article.
-
Real-world long-term outcomes in individuals at clinical risk for psychosis: The case for extending duration of care.EClinicalMedicine. 2020 Oct 7;28:100578. doi: 10.1016/j.eclinm.2020.100578. eCollection 2020 Nov. EClinicalMedicine. 2020. PMID: 33294806 Free PMC article.
-
Real-world digital implementation of the Psychosis Polyrisk Score (PPS): A pilot feasibility study.Schizophr Res. 2020 Dec;226:176-183. doi: 10.1016/j.schres.2020.04.015. Epub 2020 Apr 24. Schizophr Res. 2020. PMID: 32340785 Free PMC article.
-
Preventive psychiatry: a blueprint for improving the mental health of young people.World Psychiatry. 2021 Jun;20(2):200-221. doi: 10.1002/wps.20869. World Psychiatry. 2021. PMID: 34002494 Free PMC article.
References
-
- Fusar-Poli P, Rocchetti M, Sardella A et al. . Disorder, not just a state of risk: meta-analysis of functioning and quality of life in subjects at high clinical risk for psychosis. Br J Psychiatry. 2015;207:198–206. - PubMed
-
- Fusar-Poli P, Byrne M, Badger S, Valmaggia LR, McGuire PK. Outreach and support in south London (OASIS), 2001–2011: ten years of early diagnosis and treatment for young individuals at high clinical risk for psychosis. Eur Psychiatry. 2013;28:315–326. - PubMed
-
- Fusar-Poli P, Rutigliano G, Stahl D et al. . Long-term validity of the At Risk Mental State (ARMS) for predicting psychotic and non-psychotic mental disorders. Eur Psychiatry. 2017;42:49–54. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
