

The association between outcome-based quality indicators for intensive care units
- PMID: 29897994
- PMCID: PMC5999279
- DOI: 10.1371/journal.pone.0198522
The association between outcome-based quality indicators for intensive care units
Abstract
Purpose: To assess and improve the effectiveness of ICU care, in-hospital mortality rates are often used as principal quality indicator for benchmarking purposes. Two other often used, easily quantifiable, quality indicators to assess the efficiency of ICU care are based on readmission to the ICU and ICU length of stay. Our aim was to examine whether there is an association between case-mix adjusted outcome-based quality indicators in the general ICU population as well as within specific subgroups.
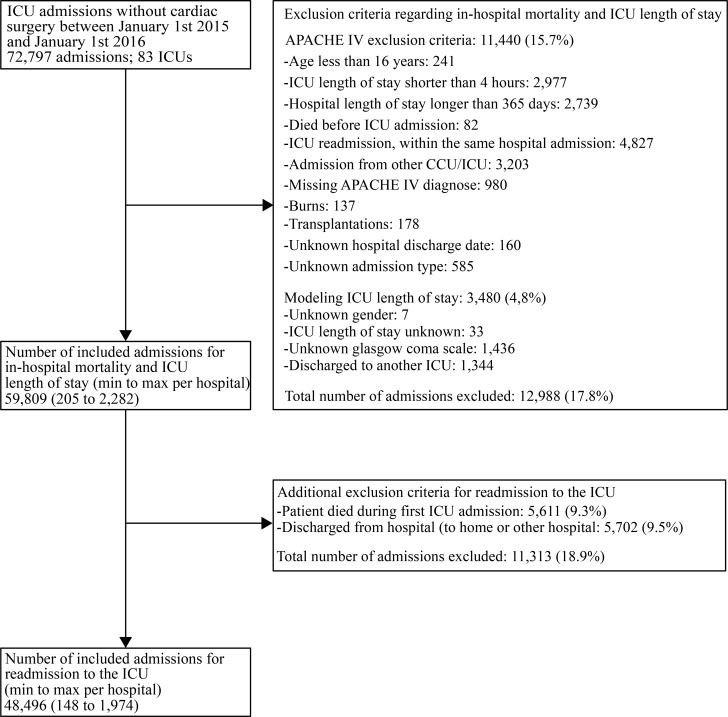
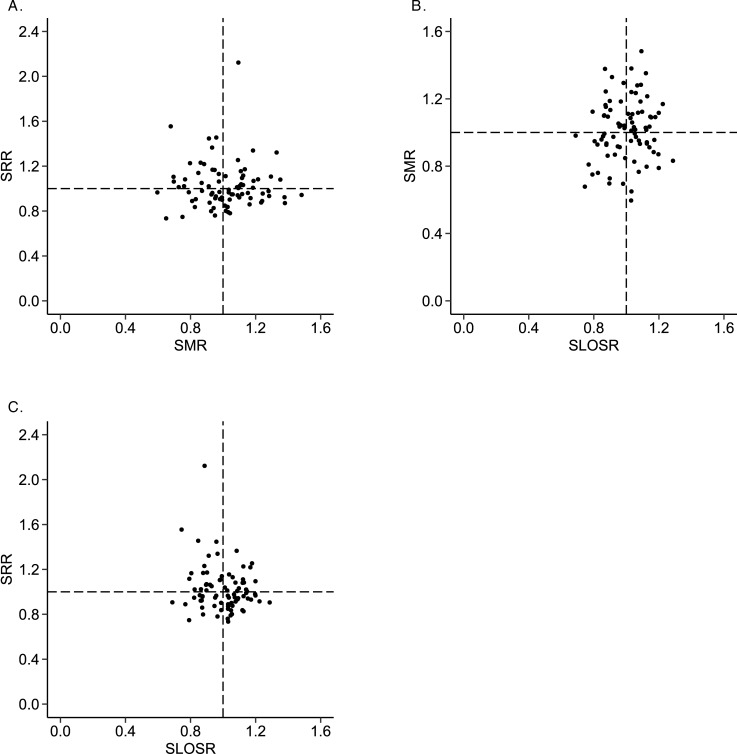
Materials and methods: We included patients admitted in 2015 of all Dutch ICUs. We derived the standardized in-hospital mortality ratio (SMR); the standardized readmission ratio (SRR); and the standardized length of stay ratio (SLOSR). We expressed association through Pearson's correlation coefficients.
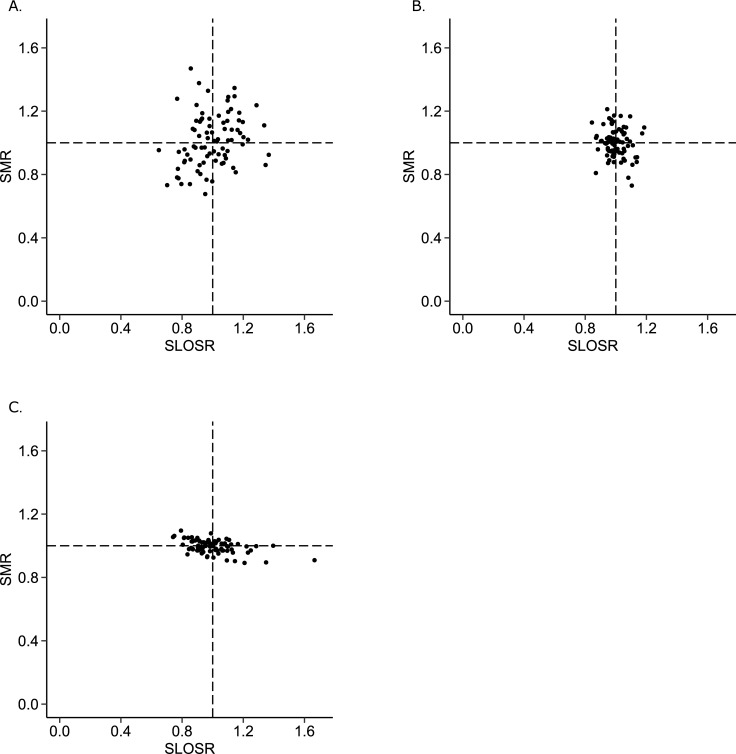
Results: The SMR ranged from 0.6 to 1.5; the SRR ranged from 0.7 to 2.1; and the SLOSR ranged from 0.7 to 1.3. For the total ICU population we found no significant associations. We found a positive, non-significant, association between SMR and SLOSR for admissions with low-mortality risk, (r = 0.25; p = 0.024), and a negative association between these indicators for admissions with high-mortality risk (r = -0.49; p<0.001).
Conclusion: Overall, we found no association at ICU population level. Differential associations were found between performance on mortality and length of stay within different risk strata. We recommend users of quality information to take these three outcome indicators into account when benchmarking ICUs as they capture different aspects of ICU performance. Furthermore, we suggest to report quality indicators for patient subgroups.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Kolfschoten NE, Kievit J, Gooiker GA, van Leersum NJ, Snijders HS, Eddes EH, et al. Focusing on desired outcomes of care after colon cancer resections; hospital variations in 'textbook outcome'. Eur J Surg Oncol. 2013;39(2):156–163. doi: 10.1016/j.ejso.2012.10.007 - DOI - PubMed
-
- Goldstein H, Spiegelhalter DJ. League Tables and Their Limitations: Statiatical Issues in Comparisons of Institutional Performance. Journal of the Royal Statistical Society 1996;159(3):358–433. doi: 10.2307/2983325 - DOI
-
- Halpern NA, Pastores SM. Critical care medicine in the United States 2000–2005: an analysis of bed numbers, occupancy rates, payer mix, and costs. Critical care medicine. 2010;38(1):65–71. doi: 10.1097/CCM.0b013e3181b090d0 - DOI - PubMed
-
- Berenholtz SM, Dorman T, Ngo K, Pronovost PJ. Qualitative review of intensive care unit quality indicators. J Crit Care. 2002;17(1):1–12. - PubMed
-
- Flaatten H. The present use of quality indicators in the intensive care unit. Acta Anaesthesiol Scand. 2012;56(9):1078–1083. doi: 10.1111/j.1399-6576.2012.02656.x - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
