

Twenty-year clinical experience with fixed functional appliances
- PMID: 29898162
- PMCID: PMC6018450
- DOI: 10.1590/2177-6709.23.2.087-109.sar
Twenty-year clinical experience with fixed functional appliances
Abstract
Introduction: Considering the large number of fixed functional appliances, choosing the best device for your patient is not an easy task.
Objective: To describe the development of fixed functional appliances as well as our 20-year experience working with them.
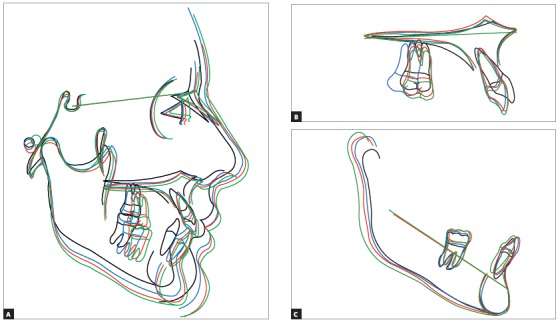
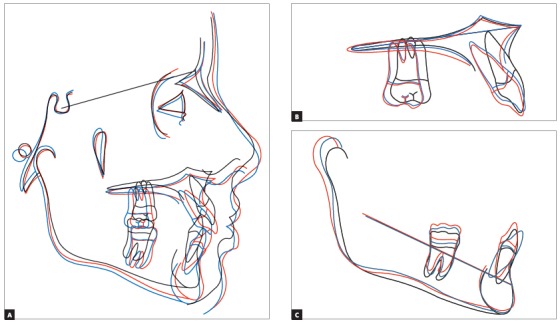
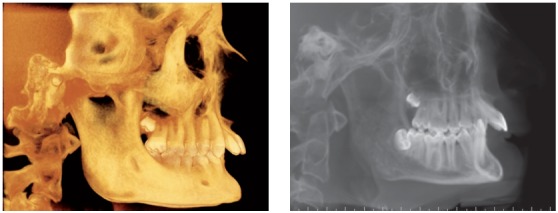
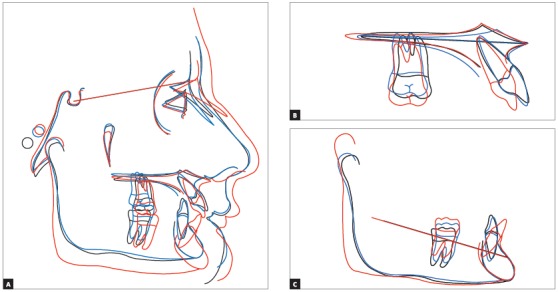
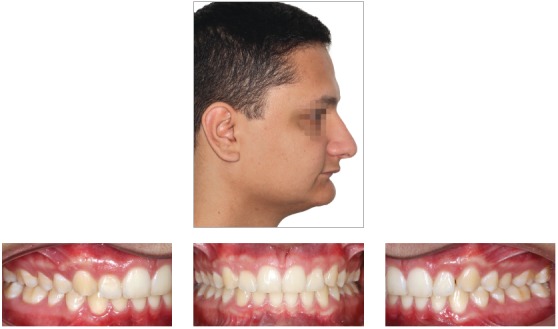
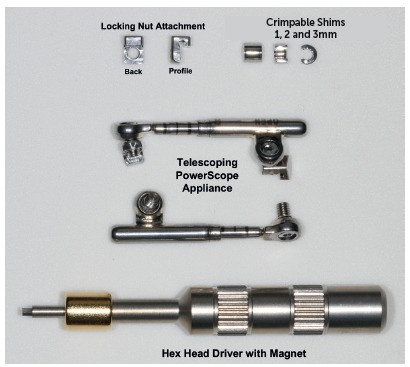
Methods: Fixed functional appliances are grouped into flexible, rigid and hybrid. They are different appliances, whose action is described here. Four clinical cases will be reported with a view to illustrating the different appliances.
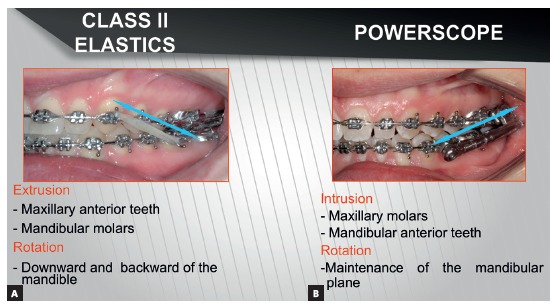
Conclusions: Rigid fixed functional appliances provide better skeletal results than flexible and hybrid ones. Flexible and hybrid appliances have similar effects to those produced by Class II elastics. They ultimately correct Class II with dentoalveolar changes. From a biomechanical standpoint, fixed functional appliances are more recommended to treat Class II in dolichofacial patients, in comparison to Class II elastics.
Introdução:: considerando-se o grande número de aparelhos propulsores mandibulares, não é uma tarefa fácil escolher o melhor deles para o seu paciente.
Objetivo:: descrever o desenvolvimento desses aparelhos e a experiência clínica de vinte anos dos autores na sua utilização.
Métodos:: os aparelhos funcionais fixos aqui apresentados foram classificados em flexíveis, rígidos e híbridos, e o modo de ação de cada um deles foi descrito e ilustrado por meio de quatro casos clínicos.
Conclusões:: os aparelhos propulsores rígidos fornecem mais resultados esqueléticos do que os flexíveis e os híbridos. Esses últimos têm efeito semelhante ao uso de elásticos com direção de Classe II e, basicamente, corrigem a má oclusão de Classe II com alterações dentoalveolares. Do ponto de vista biomecânico, os propulsores fixos estão mais indicados para tratar a Classe II em pacientes dolicofaciais do que os elásticos de Classe II.
Figures

























References
-
- Hanks SD. Trying to get out of the 20th century: a partial translation of Emil Herbst's 1910 text. World J Orthod. 2000;1(1):9–16.
-
- Pancherz H. Treatment of Class II malocclusion by jumping the bite with the Herbst appliance a cephalometric investigation. Am J Orthod. 1979;76(4):423–442. - PubMed
-
- Ritto AK, Ferreira AP. Fixed functional appliances--a classification. Funct Orthod. 2000;17(2):12–30. - PubMed
-
- Foncatti CF, Castanha Henriques JF, Janson G, Caldas W, Garib DG. Long-term stability of Class II treatment with the Jasper jumper appliance. Am J Orthod Dentofacial Orthop. 2017;152(5):663–671. - PubMed
-
- Coelho CM., Filho Mandibular protraction appliances for Class II treatment. J Clin Orthod. 1995;29(5):319–336. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
