

Association of Patient Perceptions of Cardiovascular Risk and Beliefs on Statin Drugs With Racial Differences in Statin Use: Insights From the Patient and Provider Assessment of Lipid Management Registry
- PMID: 29898219
- PMCID: PMC6656582
- DOI: 10.1001/jamacardio.2018.1511
Association of Patient Perceptions of Cardiovascular Risk and Beliefs on Statin Drugs With Racial Differences in Statin Use: Insights From the Patient and Provider Assessment of Lipid Management Registry
Abstract
Importance: African American individuals face higher atherosclerotic cardiovascular disease risk than white individuals; reasons for these differences, including potential differences in patient beliefs regarding preventive care, remain unknown.
Objective: To evaluate differences in statin use between white and African American patients and identify the potential causes for any observed differences.
Design, setting, and participants: Using the 2015 Patient and Provider Assessment of Lipid Management (PALM) Registry data, we compared statin use and dosing between African American and white outpatient adults who were potentially eligible for primary or secondary prevention statins. A total of 138 US community health care practices contributed to the data. Data analysis was conducted from March 2017 to May 2018.
Main outcomes and measures: Primary outcomes were use and dosing of statin therapy according to the 2013 American College of Cardiology/American Heart Association guideline by African American or white race. Secondary outcomes included lipid levels and patient-reported beliefs. Poisson regression was used to evaluate the association between race and statin undertreatment, a category combining people who were not taking a statin or those taking a dose intensity lower than recommended.
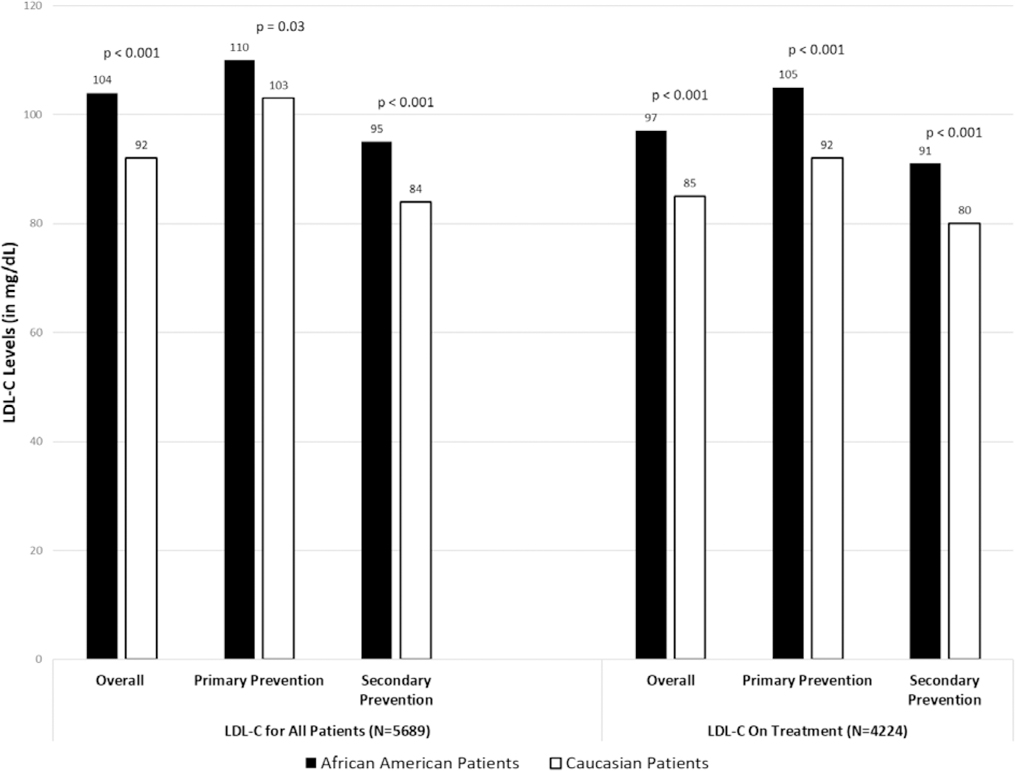
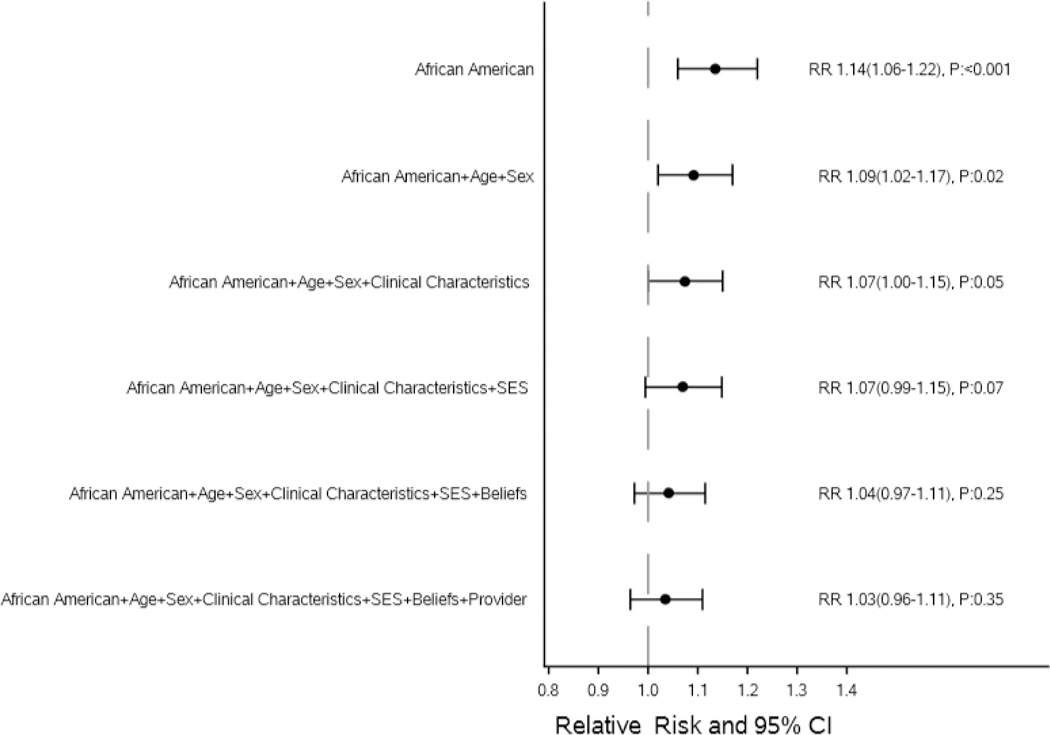
Results: A total of 5689 patients (806 [14.2%] African American) in the PALM registry were eligible for statin therapy. African American individuals were less likely than white individuals to be treated with a statin (570/807 [70.6%] vs 3654/4883 [74.8%]; P = .02). Among those treated, African American patients were less likely than white patients to receive a statin at guideline-recommended intensity (269 [33.3%] vs 2145 [43.9%], respectively; P < .001; relative risk, 1.07 [95% CI, 1.00-1.15]; P = .05, after adjustment for demographic and clinical factors). The median (interquartile range) low-density lipoprotein cholesterol levels of patients receiving treatment were higher among African American than white individuals (97.0 [76.0-121.0] mg/dL vs 85.0 [68.0-105.0] mg/dL; P < .001). African American individuals were less likely than white individuals to believe statins were safe (292 [36.2%] vs 2800 [57.3%]; P < .001) or effective (564 [70.0%] vs 3635 [74.4%]; P = .008) and were less likely to trust their clinician (663 [82.3%] vs 4579 [93.8%]; P < .001). Group differences in statin undertreatment were not significant after adjusting for demographic, clinical, and clinician factors, socioeconomic status, and patient beliefs (final adjusted relative risk, 1.03 [95% CI 0.96-1.11]; P = .35).
Conclusions and relevance: African American individuals were less likely to receive guideline-recommended statin therapy. Demographic, clinical, socioeconomic, belief-related, and clinician differences contributed to observed differences and represent potential targets for intervention.
Conflict of interest statement
Conflict of Interest Disclosures
Figures

Comment in
-
Addressing Cardiovascular Disease Disparities-Are We Getting Closer to the Truth?JAMA Cardiol. 2018 Aug 1;3(8):748. doi: 10.1001/jamacardio.2018.1510. JAMA Cardiol. 2018. PMID: 29898216 No abstract available.
References
-
- Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S1–45. - PubMed
-
- Writing Group Members, Mozaffarian D, Benjamin EJ, et al. Heart Disease and Stroke Statistics-2016 Update: a report from the American Heart Association. Circulation. 2016;133(4):e38–360. - PubMed
-
- Mann D, Reynolds K, Smith D, Muntner P. Trends in statin use and low-density lipoprotein cholesterol levels among US adults: impact of the 2001 National Cholesterol Education Program guidelines. Ann Pharmacother. 2008;42(9):1208–1215. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
