

What do we know about frailty in the acute care setting? A scoping review
- PMID: 29898673
- PMCID: PMC6000922
- DOI: 10.1186/s12877-018-0823-2
What do we know about frailty in the acute care setting? A scoping review
Abstract
Background: The ability of acute care providers to cope with the influx of frail older patients is increasingly stressed, and changes need to be made to improve care provided to older adults. Our purpose was to conduct a scoping review to map and synthesize the literature addressing frailty in the acute care setting in order to understand how to tackle this challenge. We also aimed to highlight the current gaps in frailty research.
Methods: This scoping review included original research articles with acutely-ill Emergency Medical Services (EMS) or hospitalized older patients who were identified as frail by the authors. We searched Medline, CINAHL, Embase, PsycINFO, Eric, and Cochrane from January 2000 to September 2015.
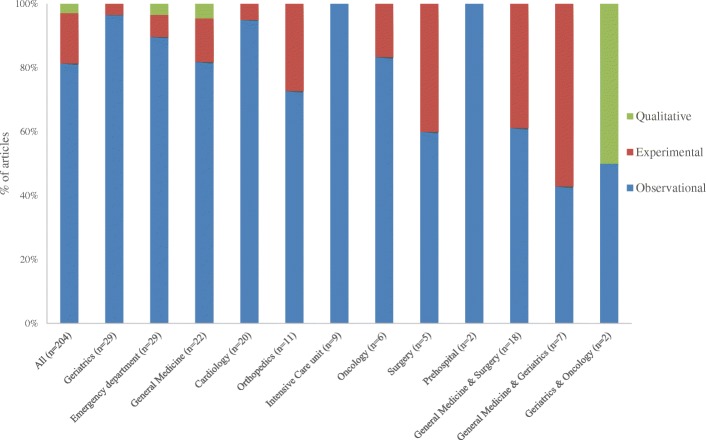
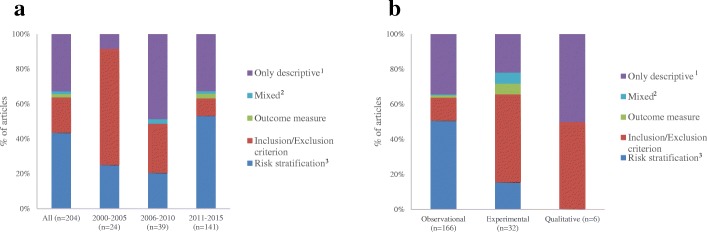
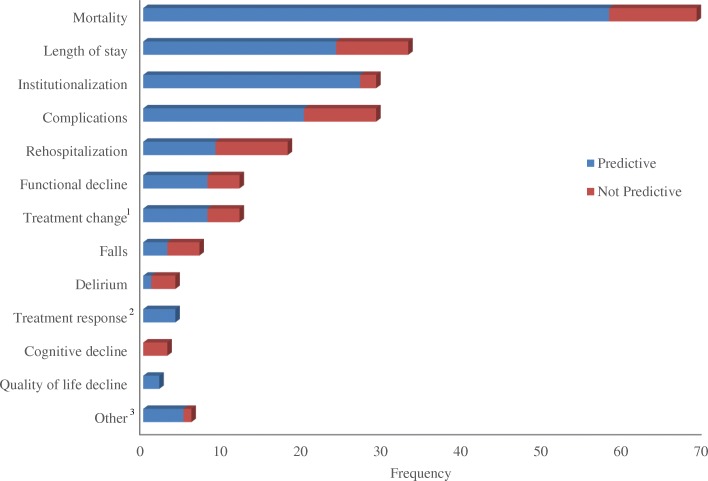
Results: Our database search initially resulted in 8658 articles and 617 were eligible. In 67% of the articles the authors identified their participants as frail but did not report on how they measured frailty. Among the 204 articles that did measure frailty, the most common disciplines were geriatrics (14%), emergency department (14%), and general medicine (11%). In total, 89 measures were used. This included 13 established tools, used in 51% of the articles, and 35 non-frailty tools, used in 24% of the articles. The most commonly used tools were the Clinical Frailty Scale, the Frailty Index, and the Frailty Phenotype (12% each). Most often (44%) researchers used frailty tools to predict adverse health outcomes. In 74% of the cases frailty predicted the outcome examined, typically mortality and length of stay.
Conclusions: Most studies (83%) were conducted in non-geriatric disciplines and two thirds of the articles identified participants as frail without measuring frailty. There was great variability in tools used and more recently published studies were more likely to use established frailty tools. Overall, frailty appears to be a good predictor of adverse health outcomes. For frailty to be implemented in clinical practice frailty tools should help formulate the care plan and improve shared decision making. How this will happen has yet to be determined.
Keywords: Acute care; Aging; Frail elderly; Frailty; Older adults; Scoping review.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Competing interests
Dr. Olga Theou, first author, is a member of the BMC Geriatrics editorial board.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Theou O, Rockwood K. Comparison and clinical applications of the frailty phenotype and frailty index approaches. Interdiscip Top Gerontol Geriatr. 2015;41:74–84. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
