

Improved short and long term survival associated with percutaneous coronary intervention in the elderly patients with acute coronary syndrome
- PMID: 29898676
- PMCID: PMC6001043
- DOI: 10.1186/s12877-018-0818-z
Improved short and long term survival associated with percutaneous coronary intervention in the elderly patients with acute coronary syndrome
Abstract
Background: Percutaneous coronary intervention (PCI) are increasingly used in daily clinical practice in elderly patients with acute coronary syndrome (ACS) despite limited evidence. The purpose of this study was to assess the impact of PCI on short and long term survivals in a large cohort of elderly patients with ACS from a "real world".
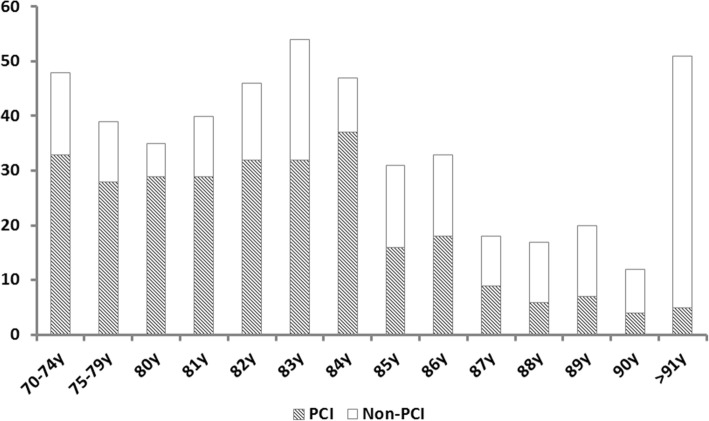
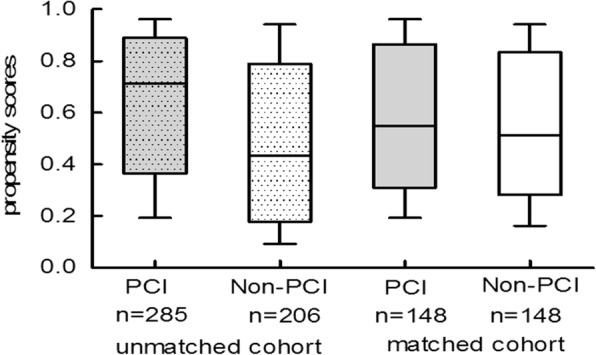
Methods: We enrolled 491 patients aged ≥70 years admitted to our institution with ACS from 2006 to 2012. Effect of PCI on short and long term survival was evaluated in both overall and a propensity score-matched cohort.
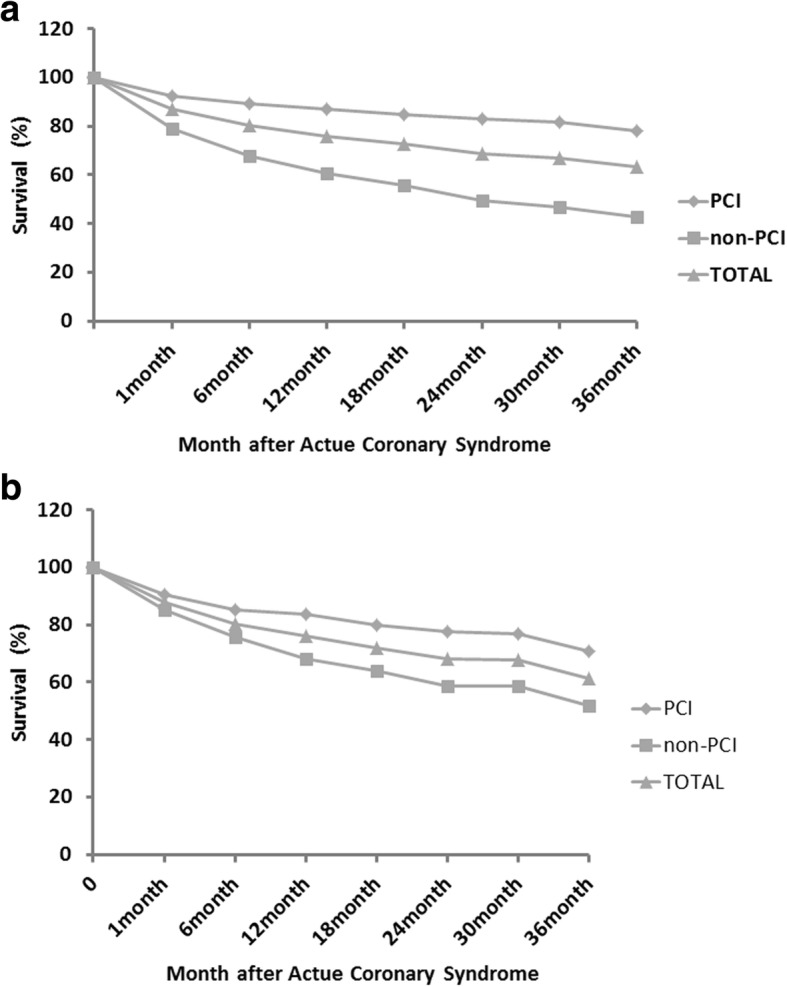
Results: The mean age of the overall cohort is 83 ± 6 years. Among them, 285 were treated with PCI, whereas 206 were not. Patients treated with PCI were younger (82 ± 5 vs. 85 ± 6), more males (67% vs. 46%), with lower heart rate (77 ± 22 vs. 84 ± 21), higher eGFR (58 ± 20 vs. 47 ± 23), and less with heart failure (29% vs. 15%) (all p < 0.001). In both overall and propensity-matched population, improved survival was associated with PCI-treatment at 1 and 3 years (p < 0.001 for all comparisons). Furthermore, by using multivariate Cox proportional-hazards regression model following factors were identified as independent predictors of 3-year all-cause mortality: age (HR 1.08, 95% CI 1.00-1.16), heart rate (HR 1.02, 95% CI 1.01-1.03), eGFR (HR 3.07, 95% CI 1.63-5.77), malignancy (HR 2.03, 95% CI 1.27-4.57), prior CABG (HR 2.033, 95% CI 1.27-4.57), medication with statin (HR 0.40, 95% CI 0.19-0.86) in PCI group, whereas age (HR 1.08, 95% CI 1.03-1.13), heart rate (HR 1.01, 95% CI 1.01-1.02), hypertension (HR 1.87, 95% CI 1.01-3.49) and using of ACEI/ARB (HR 0.46, 95% CI 0.28-0.76) in non-PCI group.
Conclusions: In elderly ACS patients, PCI-treatment was associated with improved 1 and 3-year survival and PCI-treated patients had different prognostic profile compared to those without PCI treatment.
Keywords: Acute coronary syndrome; Elderly; Percutaneous coronary intervention; Short and long outcome.
Conflict of interest statement
Ethics approval and consent to participate
This study protocol was approved by the Human Ethical Committee at University of Gothenburg. All study participants provided written informed consent.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Alexander KP, Newby LK, Armstrong PW, Cannon CP, Gibler WB, Rich MW, et al. Acute coronary care in the elderly, part II: ST-segment-elevation myocardial infarction: a scientific statement for healthcare professionals from the American Heart Association Council on clinical cardiology: in collaboration with the Society of Geriatric Cardiology. Circulation. 2007;115:2570–2589. doi: 10.1161/CIRCULATIONAHA.107.182616. - DOI - PubMed
-
- Alexander KP, Newby LK, Cannon CP, Armstrong PW, Gibler WB, Rich MW, et al. Acute coronary care in the elderly, part I: non-ST-segment-elevation acute coronary syndromes: a scientific statement for healthcare professionals from the American Heart Association Council on clinical cardiology: in collaboration with the Society of Geriatric Cardiology. Circulation. 2007;115:2549–2569. doi: 10.1161/CIRCULATIONAHA.107.182615. - DOI - PubMed
-
- Force m A/T, Windecker S, Kolh P, Alfonso F, Collet JP, Cremer J, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: the task force on myocardial revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI) Eur Heart J. 2014;35:2541–2619. doi: 10.1093/eurheartj/ehu278. - DOI - PubMed
-
- Dzavik V, Sleeper LA, Cocke TP, Moscucci M, Saucedo J, Hosat S, et al. Early revascularization is associated with improved survival in elderly patients with acute myocardial infarction complicated by cardiogenic shock: a report from the SHOCK trial registry. Eur Heart J. 2003;24:828–837. doi: 10.1016/S0195-668X(02)00844-8. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
