

Patient care activities by community pharmacists in a capitation funding model mental health and addictions program
- PMID: 29898682
- PMCID: PMC6000927
- DOI: 10.1186/s12888-018-1746-3
Patient care activities by community pharmacists in a capitation funding model mental health and addictions program
Abstract
Background: Community pharmacists are autonomous, regulated health care professionals located in urban and rural communities in Canada. The accessibility, knowledge, and skills of community pharmacists can be leveraged to increase mental illness and addictions care in communities.
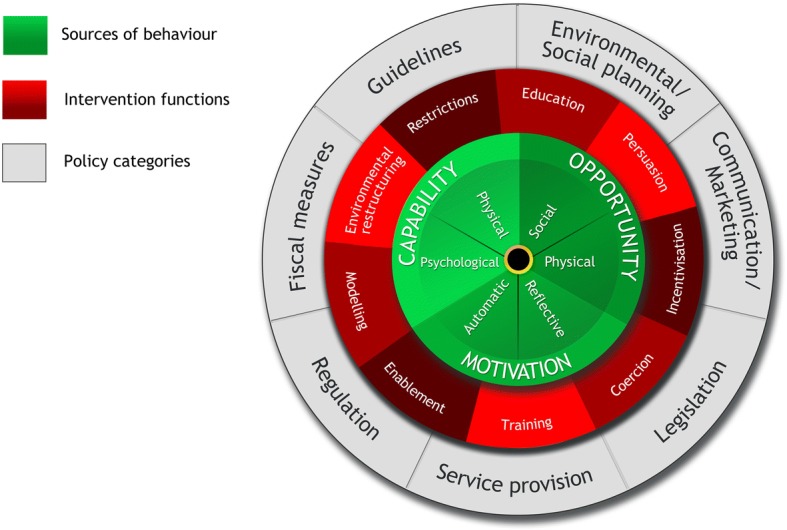
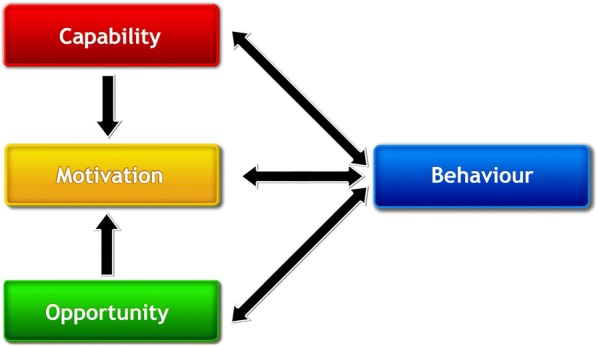
Methods: The Bloom Program was designed, developed, and implemented based on the Behaviour Change Wheel and a program of research in community pharmacy mental healthcare capacity building. We evaluated the Bloom Program as a demonstration project using mixed methods. A retrospective chart audit was conducted to examine outcomes and these are reported in this paper.
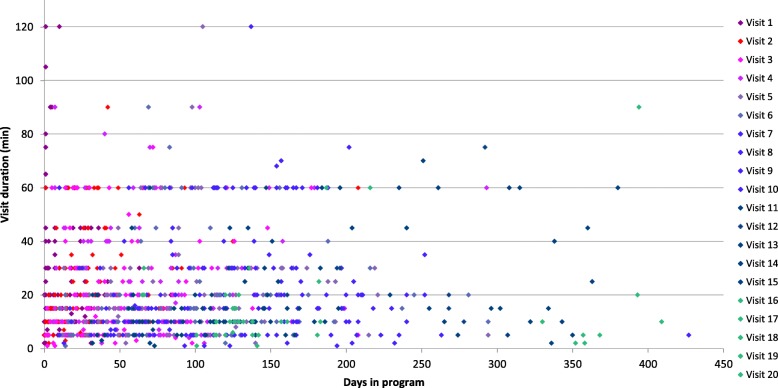
Results: We collected 201 patient charts from 23 pharmacies in Nova Scotia with 182 patients having at least one or more follow-up visits. Anxiety (n = 126, 69%), depression (n = 112, 62%), and sleep disorders (n = 64, 35%) were the most frequent mental health problems. Comorbid physical health problems were documented in 57% (n = 104). The average number of prescribed medications was 5.5 (range 0 to 24). Sixty seven percent (n = 122) were taking multiple psychotropics and 71% (n = 130) reported taking more than one medication for physical health problems. Treatment optimization was the leading reason for enrollment with more than 80% seeking improvements in symptom management and daily functioning. There were a total of 1233 patient-care meetings documented, of which the duration was recorded in 1098. The median time for enrolling, assessing, and providing follow-up care by pharmacists was 142 min (mean 176, SD 128) per patient. The median follow-up encounter duration was 15 min. A total of 146 patient care encounters were 60 min or longer, representing 13.3% of all timed encounters.
Conclusions: Pharmacists work with patients with lived experience of mental illness and addictions to improve medication related outcomes including those related to treatment optimization, reducing polytherapy, and facilitating withdrawal from medications. Pharmacists can offer their services frequently and routinely without the need for an appointment while affording patient confidentiality and privacy. Important roles for pharmacists around the deprescribing of various medications (e.g., benzodiazepines) have previously been supported and should be optimized and more broadly implemented. Further research on the best mechanisms to incentivize pharmacists in mental illness and addiction's care should be explored.
Keywords: Community pharmacy services; Mental disorders; Observational study; Pharmacists.
Conflict of interest statement
Authors’ information
ALM and DMG are academic faculty at Dalhousie University, Halifax, Nova Scotia, Canada. LMJ is an independent program evaluator in Halifax, NS. Our research program is focused on designing, developing, and implementing interventions for community pharmacists caring for people with lived experience of mental illness and addictions in primary health care.
Ethics approval and consent to participate
Dalhousie University Research Ethics Board reviewed the demonstration project proposal and ethics submission and determined that it constituted program evaluation. A formal ethics review was therefore not provided. A privacy impact assessment was completed and approved by the government of Nova Scotia in accordance with provincial privacy legislation.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- International Pharmaceutical Federation (FIP) Focus on mental health: the contribution of the pharmacist. 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
