

Does clinician-reported lipid guideline adoption translate to guideline-adherent care? An evaluation of the Patient and Provider Assessment of Lipid Management (PALM) registry
- PMID: 29898839
- PMCID: PMC6526059
- DOI: 10.1016/j.ahj.2018.03.011
Does clinician-reported lipid guideline adoption translate to guideline-adherent care? An evaluation of the Patient and Provider Assessment of Lipid Management (PALM) registry
Abstract
Background: The 2013 American College of Cardiology (ACC)/American Heart Association (AHA) cholesterol guideline recommends statin treatment based on patients' predicted atherosclerotic cardiovascular disease (ASCVD) risk. Whether clinician-reported guideline adoption translates to implementation into practice is unknown.
Objectives: We aimed to compare clinician lipid management in hypothetical scenarios versus observed practice.
Methods: The PALM Registry asked 774 clinicians how they would treat 4 hypothetical scenarios of primary prevention patients with: (1) diabetes; (2) high 10-year ASCVD risk (≥7.5%) with high low-density lipoprotein cholesterol (LDL-C; ≥130 mg/dL); (3) low 10-year ASCVD risk (<7.5%) with high LDL-C (130-189 mg/dL); or (4) primary and secondary prevention patients with persistently elevated LDL-C (≥130 mg/dL) despite high-intensity statin use. We assessed agreement between clinician survey responses and observed practice.
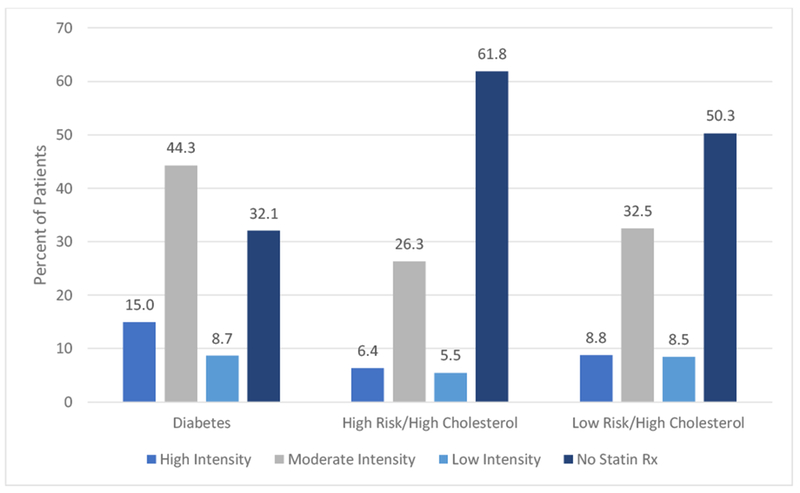
Results: In primary prevention scenarios, 85% of clinicians reported they would prescribe a statin to a diabetic patient and 93% to a high-risk/high LDL-C patient (both indicated by guidelines), while 40% would prescribe statins to a low-risk/high LDL-C patient. In clinical practice, statin prescription rates were 68% for diabetic patients, 40% for high-risk/high LDL-C patients, and 50% for low-risk/high LDL-C patients. Agreement between hypothetical and observed practice was 64%, 39%, and 52% for patients with diabetes, high-risk/high LDL-C, and low-risk/high LDL-C, respectively. Among patients with persistently high LDL-C despite high-intensity statin treatment, 55% of providers reported they would add a non-statin lipid-lowering medication, while only 22% of patients were so treated.
Conclusions: While the majority of clinicians report adoption of the 2013 ACC/AHA guideline recommendations, observed lipid management decisions in practice are frequently discordant.
Copyright © 2018 Elsevier Inc. All rights reserved.
Figures
References
-
- Chou R, Dana T, Blazina I, Daeges M, Jeanne TL. Statins for Prevention of Cardiovascular Disease in Adults: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2016;316:2008–2024. - PubMed
-
- Ray KK, Cannon CP, McCabe CH et al. Early and late benefits of high-dose atorvastatin in patients with acute coronary syndromes: results from the PROVE IT-TIMI 22 trial. J Am Coll Cardiol 2005;46:1405–10. - PubMed
-
- Pedersen TR, Faergeman O, Kastelein JJ et al. High-dose atorvastatin vs usual-dose simvastatin for secondary prevention after myocardial infarction: the IDEAL study: a randomized controlled trial. JAMA 2005;294:2437–45. - PubMed
-
- LaRosa JC, Grundy SM, Waters DD et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. The New England journal of medicine 2005;352:1425–35. - PubMed
-
- Cannon CP, Blazing MA, Giugliano RP et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. The New England journal of medicine 2015;372:2387–97. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
