

Elective Nodal Irradiation Attenuates the Combinatorial Efficacy of Stereotactic Radiation Therapy and Immunotherapy
- PMID: 29898992
- PMCID: PMC6532976
- DOI: 10.1158/1078-0432.CCR-17-3427
Elective Nodal Irradiation Attenuates the Combinatorial Efficacy of Stereotactic Radiation Therapy and Immunotherapy
Abstract
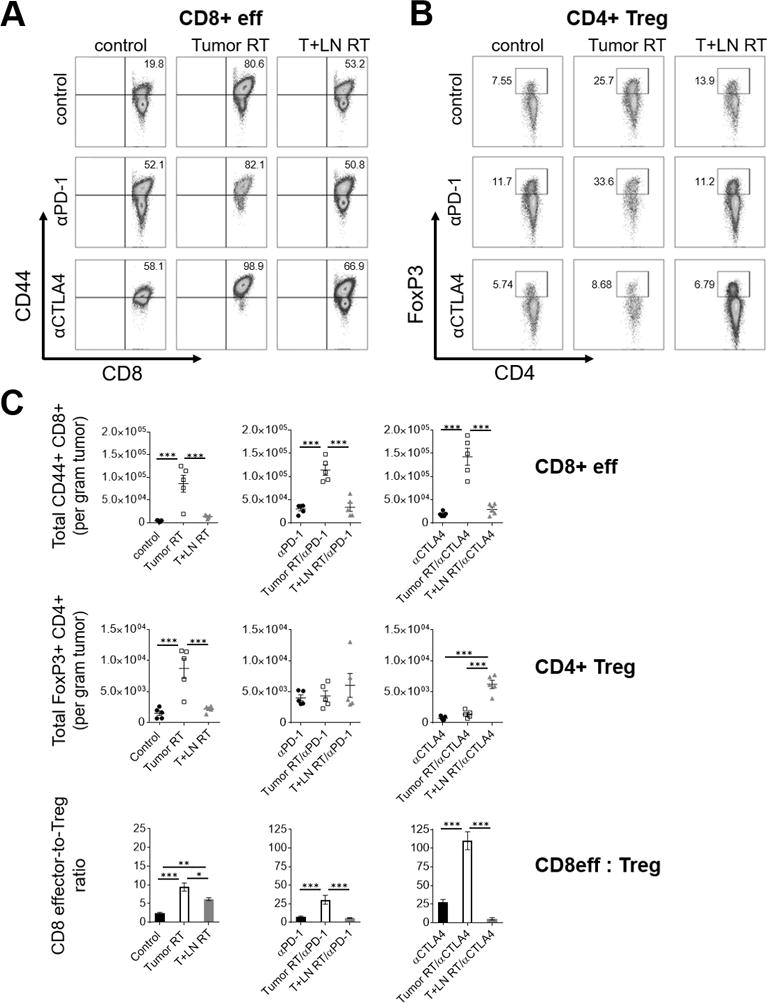
Purpose: In the proper context, radiotherapy can promote antitumor immunity. It is unknown if elective nodal irradiation (ENI), a strategy that irradiates tumor-associated draining lymph nodes (DLN), affects adaptive immune responses and combinatorial efficacy of radiotherapy with immune checkpoint blockade (ICB).Experimental Design: We developed a preclinical model to compare stereotactic radiotherapy (Tumor RT) with or without ENI to examine immunologic differences between radiotherapy techniques that spare or irradiate the DLN.Results: Tumor RT was associated with upregulation of an intratumoral T-cell chemoattractant chemokine signature (CXCR3, CCR5-related) that resulted in robust infiltration of antigen-specific CD8+ effector T cells as well as FoxP3+ regulatory T cells (Tregs). The addition of ENI attenuated chemokine expression, restrained immune infiltration, and adversely affected survival when combined with ICB, especially with anti-CLTA4 therapy. The combination of stereotactic radiotherapy and ICB led to long-term survival in a subset of mice and was associated with favorable CD8 effector-to-Treg ratios and increased intratumoral density of antigen-specific CD8+ T cells. Although radiotherapy technique (Tumor RT vs. ENI) affected initial tumor control and survival, the ability to reject tumor upon rechallenge was partially dependent upon the mechanism of action of ICB; as radiotherapy/anti-CTLA4 was superior to radiotherapy/anti-PD-1.Conclusions: Our results highlight that irradiation of the DLN restrains adaptive immune responses through altered chemokine expression and CD8+ T-cell trafficking. These data have implications for combining radiotherapy and ICB, long-term survival, and induction of immunologic memory. Clinically, the immunomodulatory effect of the radiotherapy strategy should be considered when combining stereotactic radiotherapy with immunotherapy. Clin Cancer Res; 24(20); 5058-71. ©2018 AACR.
©2018 American Association for Cancer Research.
Conflict of interest statement
Figures






References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
