

Triple negative breast cancer subtypes and pathologic complete response rate to neoadjuvant chemotherapy
- PMID: 29899867
- PMCID: PMC5995183
- DOI: 10.18632/oncotarget.25413
Triple negative breast cancer subtypes and pathologic complete response rate to neoadjuvant chemotherapy
Abstract
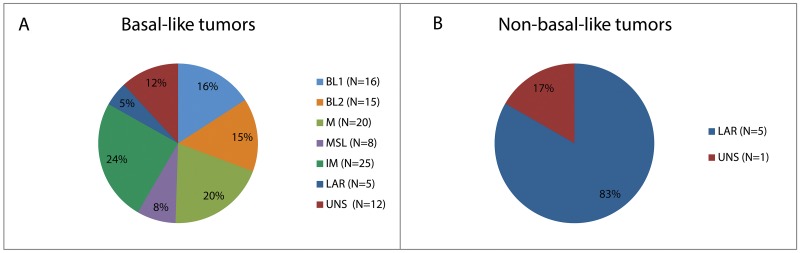
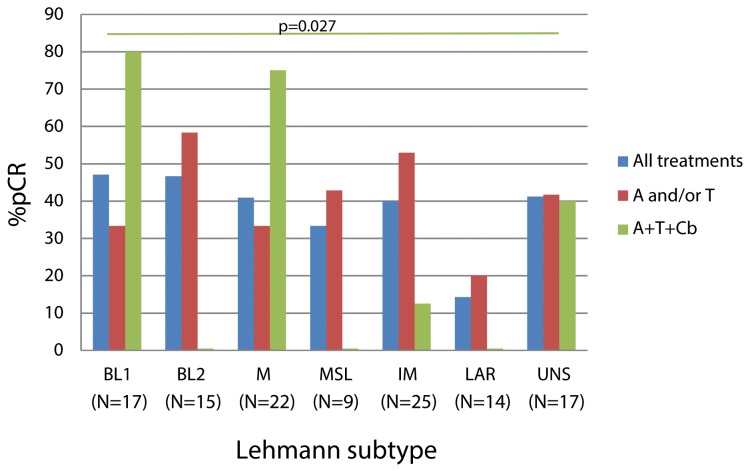
Triple negative breast cancer (TNBC) is a heterogeneous disease with distinct molecular subtypes that differentially respond to chemotherapy and targeted agents. The purpose of this study is to explore the clinical relevance of Lehmann TNBC subtypes by identifying any differences in response to neoadjuvant chemotherapy among them. We determined Lehmann subtypes by gene expression profiling in paraffined pre-treatment tumor biopsies from 125 TNBC patients treated with neoadjuvant anthracyclines and/or taxanes +/- carboplatin. We explored the clinicopathological characteristics of Lehmann subtypes and their association with the pathologic complete response (pCR) to different treatments. The global pCR rate was 37%, and it was unevenly distributed within Lehmann's subtypes. Basal-like 1 (BL1) tumors exhibited the highest pCR to carboplatin containing regimens (80% vs 23%, p=0.027) and were the most proliferative (Ki-67>50% of 88.2% vs. 63.7%, p=0.02). Luminal-androgen receptor (LAR) patients achieved the lowest pCR to all treatments (14.3% vs 42.7%, p=0.045 when excluding mesenchymal stem-like (MSL) samples) and were the group with the lowest proliferation (Ki-67≤50% of 71% vs 27%, p=0.002). In our cohort, only tumors with LAR phenotype presented non-basal-like intrinsic subtypes (HER2-enriched and luminal A). TNBC patients present tumors with a high genetic diversity ranging from highly proliferative tumors, likely responsive to platinum-based therapies, to a subset of chemoresistant tumors with low proliferation and luminal characteristics.
Keywords: carboplatin; neoadjuvant therapy; pathologic complete response; subtyping; triple negative breast cancer.
Conflict of interest statement
CONFLICTS OF INTEREST The authors declare that they have no conflicts of interest.
Figures
References
-
- Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA, Lickley LA, Rawlinson E, Sun P, Narod SA. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007;13:4429–34. - PubMed
-
- Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010;363:1938–48. - PubMed
-
- von Minckwitz G, Loibl S, Maisch A, Untch M. Lessons from the neoadjuvant setting on how best to choose adjuvant therapies. The Breast. 2011;20:S142–5. - PubMed
-
- Wang-Lopez Q, Chalabi N, Abrial C, Radosevic-Robin N, Durando X, Mouret-Reynier MA, Benmammar KE, Kullab S, Bahadoor M, Chollet P, Penault-Llorca F, Nabholtz JM. Can pathologic complete response (pCR) be used as a surrogate marker of survival after neoadjuvant therapy for breast cancer? Crit Rev Oncol Hematol. 2015;95:88–104. - PubMed
-
- Liedtke C, Mazouni C, Hess KR, André F, Tordai A, Mejia JA, Symmans WF, Gonzalez-Angulo AM, Hennessy B, Green M, Cristofanilli M, Hortobagyi GN, Pusztai L. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol. 2008;26:1275–81. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
