

Derotational Osteotomy of the Distal Femur for the Treatment of Patellofemoral Instability Simultaneously Leads to the Correction of Frontal Alignment: A Laboratory Cadaveric Study
- PMID: 29900182
- PMCID: PMC5985607
- DOI: 10.1177/2325967118775664
Derotational Osteotomy of the Distal Femur for the Treatment of Patellofemoral Instability Simultaneously Leads to the Correction of Frontal Alignment: A Laboratory Cadaveric Study
Abstract
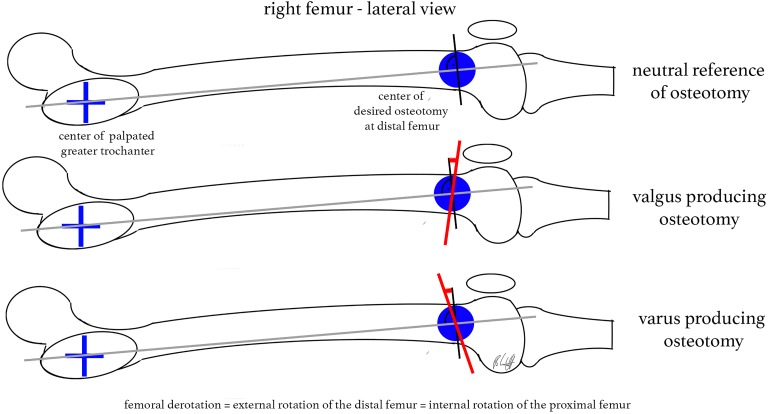
Background: Derotational osteotomy of the distal femur allows the anatomic treatment of patellofemoral maltracking due to increased femoral antetorsion. However, such rotational osteotomy procedures have a high potential of intended/unintended changes of frontal alignment.
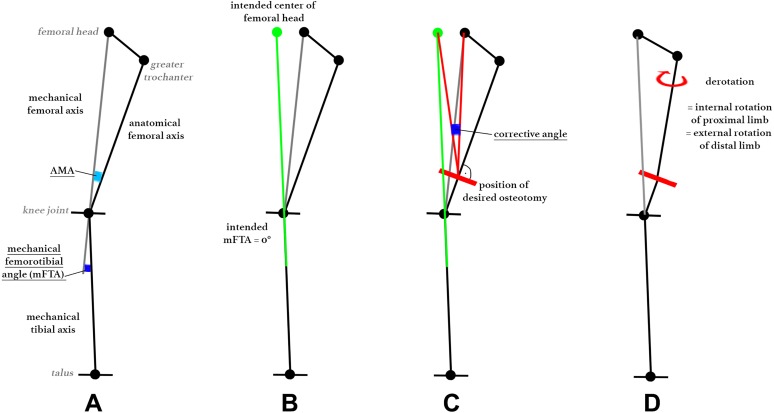
Purpose/hypothesis: The purpose of this study was to perform derotational osteotomy of the distal femur and to demonstrate the utility of a novel trigonometric approach to address 3-dimensional (3D) changes on 2-dimensional imaging (axial computed tomography [CT] and frontal-plane radiography). The hypothesis was that 1-step single-cut osteotomy can simultaneously correct torsion and frontal alignment based on preoperatively calculated cutting angles.
Study design: Controlled laboratory study.
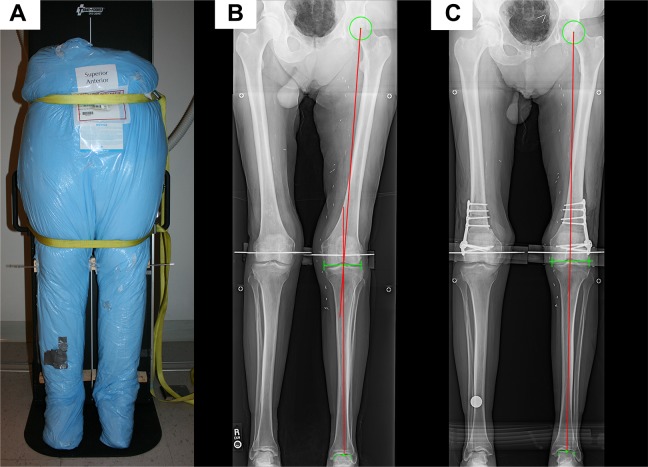
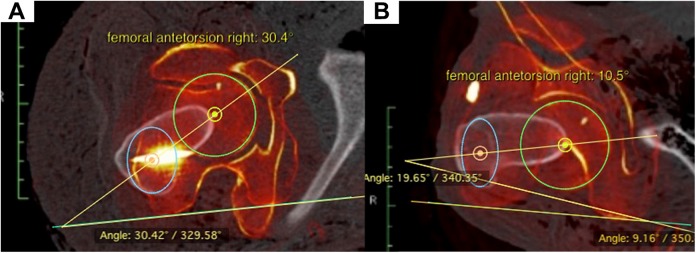
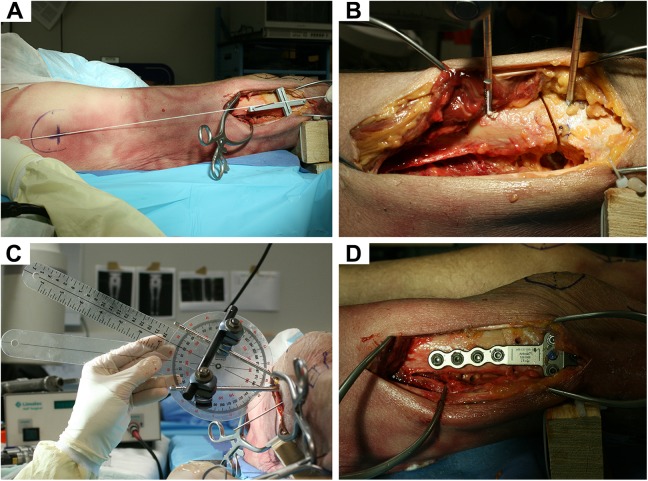
Methods: Eight human cadaveric whole legs (4 lower limb torsos) underwent derotational osteotomy of the distal femur of 20°. A straight leg axis, determined as a mechanical femorotibial angle (mFTA) of 0°, was chosen as a goal for postoperative frontal alignment. The inclination of the cutting angle from the lateral view was calculated individually for each cadaveric leg and was represented by a simple 3D-printed cutting guide for surgery. Specimens underwent CT for the measurement of torsion, while the frontal leg axis was determined on an upright radiograph preoperatively and postoperatively. Preoperative and postoperative angles were compared with the mathematical prediction model.
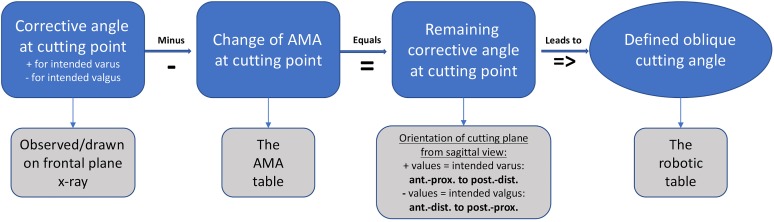
Results: The preoperative mFTA ranged from -3.9° (valgus) to +3.4° (varus) (mean, -0.2° ± 2.6°). A postoperative mean mFTA of 0.37° ± 0.69° (95% CI, -0.22° to 0.95°) was achieved (P = .01). Derotation showed a mean of 19.1° ± 2.1° (95% CI, 17.3°-20.8°). The oblique cutting plane for the correction of valgus legs showed a mean of 5.9° ± 6.8° and, for the correction of varus legs, a mean of -10.0° ± 4.5° projected on the perpendicular plane to the virtual anatomic shaft axis from the sagittal view.
Conclusion: Single-cut distal femoral osteotomy can be performed to simultaneously address rotational as well as frontal alignment using a preoperatively defined oblique cut, as determined by the presented reproducible calculation model.
Clinical relevance: This study adds important knowledge to the technique of derotational osteotomy. This approach provides an individual, oblique single cut for the correction of torsion and frontal axis within a clinically insignificant margin. Simplified tables for calculation and a surgical reference make this model reproducible and safe.
Keywords: 3D printing; distal femoral derotational osteotomy; femoral antetorsion; patellofemoral instability; torsion correction; valgus-varus alignment.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: The University of Connecticut Health Center/UConn Musculoskeletal Institute has received direct funding and material support from Arthrex for this study; the company had no influence on the study design, data collection, or interpretation of the results or the final article. Additionally, this work was supported by the German Research Foundation and the Technical University of Munich within the funding program Open Access Publishing. K.B. is a consultant for Arthrex. A.D.M. is a consultant for Orthofix and Arthrex and has received research grants from Arthrex. R.A.A. has received educational and institutional grants from Arthrex and is a consultant for Biorez. A.B.I. is a consultant for Arthrosurface, Arthrex, and medi Bayreuth.
Figures
References
-
- Brattström H. Shape of the intercondylar groove normally and in recurrent dislocation of patella: a clinical and x-ray anatomical investigation. Acta Orthop Scand. 1964;35(suppl 68):1–148. - PubMed
-
- Cahue S, Dunlop D, Hayes K, Song J, Torres L, Sharma L. Varus-valgus alignment in the progression of patellofemoral osteoarthritis. Arthritis Rheum. 2004;50(7):2184–2190. - PubMed
-
- Delgado ED, Schoenecker PL, Rich MM, Capelli AM. Treatment of severe torsional malalignment syndrome. J Pediatr Orthop. 1996;16(4):484–488. - PubMed
-
- Dickschas J, Harrer J, Bayer T, Schwitulla J, Strecker W. Correlation of the tibial tuberosity-trochlear groove distance with the Q-angle. Knee Surg Sports Traumatol Arthrosc. 2016;24(3):915–920. - PubMed
-
- Dickschas J, Harrer J, Pfefferkorn R, Strecker W. Operative treatment of patellofemoral maltracking with torsional osteotomy. Arch Orthop Trauma Surg. 2012;132(3):289–298. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
